
Abstract
Background:
The counselors’ form the backbone of HIV/AIDS control program, and for voluntary counseling and testing services to be effective counselors’ opinions are crucial.
Purpose:
To assess the perceptions of integrated counseling and testing center (ICTC) counselors with respect to the training received, problems faced in providing services, and job satisfaction.
Methods:
Qualitative methods such as 1 focus group discussion and 7 in-depth interviews were conducted among 14 counselors employed at 13 ICTCs in a costal district of south India.
Results:
The counselors identified the need for improving refresher training; job perception and satisfaction among counselors was found to be poor; issues such as shared confidentiality and targets for counseling were perceived to affect the ICTC services.
Conclusion:
The issues identified by counselors such as problems related to refresher training, targets set for counseling and testing, the pay scale and shared confidentiality should be addressed for better service delivery.
Background
India has the third largest number of people living with HIV/AIDS, and an estimated 2.39 million people affected by it. 1 Voluntary counseling and testing centers (VCTCs) and Prevention of parent-to-child transmission centers (PPTCTs) for HIV were started in 1997 under the National Aids Control Program (NACP), phase I. During the NACP phase III, VCTCs and PPTCTs were integrated to provide services under the same roof as integrated counseling and testing centers (ICTCs). 2 According to the National AIDS Control Organizations (NACO) annual report 2010 to 2011, there are 5233 ICTCs functioning under NACP III and a total of 11 158 869 clients have undergone counseling. 1 For the year 2010 to 2011, the targets set for counseling and testing in India by NACO were 11 171 000 for general clients (men and women other than pregnant women) and 8 649 500 for pregnant women. 1
The ICTC is managed by a team comprised of an ICTC manager (medical officer), a counselor, and a laboratory technician. Counselors at the ICTC provide information on HIV prevention and related health education; psychosocial support; appropriate referrals; and support, logistics, and monitoring. 3 Hence, among the ICTC staff, counselors form the backbone of the HIV/AIDS control program. A report by Rachier et al has suggested that for voluntary counseling and testing services to be effective, counselors’ opinions are crucial but are rarely consulted for their professional opinion. 4 Study conducted among HIV/AIDS counselors in Kenya and Tanzania found that counselors perceived a pressure to be role models in the community. The “spillover” of HIV issues from their personal lives caused additional stress compounded by economic and political issues. 5 Another study conducted by Kabbash et al in Egypt identified a lack of administrative support, unclear working rules and regulations, lack of proper community awareness, the need for further training, the need for a fixed job description, and improved working environment to ensure privacy and confidentiality. 6 Ginwalla et al conducted a study among nurse counselors and community volunteers and emphasized the need for training counselors. 7 The objective of our study was to assess the perceptions of counselors with respect to training received, problems faced in providing services, and job satisfaction. The information obtained following this study could be utilized to improve service delivery at ICTCs. 4
Methodology
The study was conducted among ICTC counselors employed at 13 centers functioning under NACP III of Udupi district. Udupi is one of the costal districts of Karnataka in South India, with a population of 1 177 908 (2011 census). 8 During the months of April to December 2010, a total of 14 129 clients were counseled at 13 ICTCs against the target of 18 839. 3 The study included all the 14 counselors employed at ICTCs of Udupi. The qualitative data were collected by 1 focus group discussion (FGD) and 7 in-depth interviews. Prior to FGD, the dates for the focus group were confirmed during the monthly meeting of the counselors. E-mails were sent to the counselors with details of the date, time, and venue. The counselors were also contacted by phone 1 day prior to the FGD. The guide was developed based on interviews with some of the counselors and with a close observation of the activities at ICTCs. The program guide broadly covered areas such as training, duties of counselors, job perception, problems faced in service delivery, and support available. The team conducting the FGD consisted of a female moderator and 2 facilitators. The FGD was conducted at the lecture hall of Kasturba Medical College, providing adequate privacy during the session. The counselors were given code numbers (eg, C1, C2, C3, etc, where “C” stands for counselor), which helped in maintaining anonymity. The moderator conducted the session, while one of the facilitators made notes, and the other made the sociogram. The session lasted for 1½ hours and was audio recorded with the consent of the counselors. In-depth interviews were conducted for the 4 male and 3 female counselors who did not participate in the FGD. Each in-depth interview lasted for 45 minutes and was audio recorded. The audio recordings from FGD and in-depth interviews were transcribed and coded based on the emerging themes; the data being presented as themes followed by a verbatim account of the counselors. Ethical clearance to conduct the study was obtained from the institutional ethics committee of Kasturba Medical College, Manipal University. Permissions were obtained from District Health Officer and District AIDS Prevention and Control Officer. Written informed consent was obtained from all the counselors.
Results
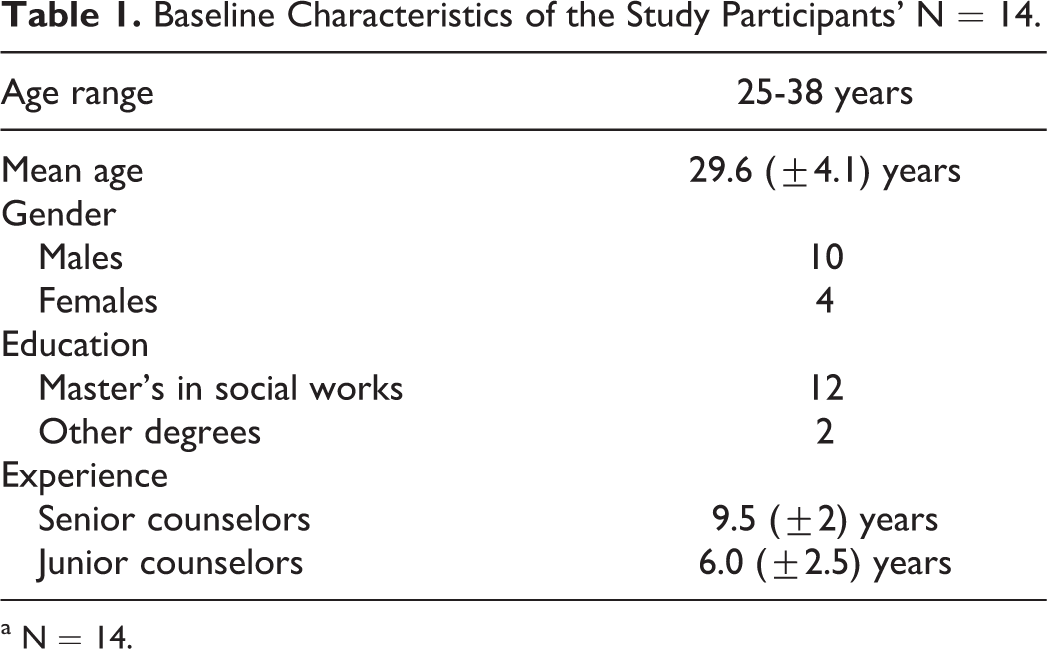
Our study included 14 counselors working at 13 ICTCs functioning under National AIDS Control Programme (NACP). The age range of the counselors was between 25 and 38 years, with a mean age of 29.64 (± 4.1). Of the 14 counselors, 10 were females. Of the 14 counselors, 12 had a master’s degree in social work, 1 with master’s in psychology, and 1 with a diploma in HIV/AIDS counseling. Six senior counselors had a mean experience of 9.5 years (standard deviation [SD] ± 1.96), whereas others had an experience of 6 years (SD ± 2.5; Table 1. The induction training received by the counselors ranged between 5 and 12 days. The 6 senior counselors received 5 to 8 days of training. Although they felt that the training they received was inadequate, they also felt that additional training was needed when they started. The other counselors rated induction training as either adequate or good. All counselors attended refresher training and majority (12 of 14) of them were not satisfied by the refresher training they received (Table 2). The factors that caused dissatisfaction were the content of training sessions, which they felt had nothing new, having to read the training manual during the sessions, unnecessary prolongation of the sessions, nongovernmental organizations (NGOs) conducting the training and colleagues as “resource persons,” who they felt had the same level of knowledge as them. Verbatim of counselor numbers 10 and 5 are presented subsequently.
Baseline Characteristics of the Study Participants’ N = 14.
a N = 14.
Perceptions of the Counselors about HIV Counseling and Testing Services.a

a n = 14.
Some of the trainers were our own colleagues and they knew only as much as we know, our own colleagues training us is very sad. (C10) We are scared of training because the same topic which starts in the morning is repeated again and again till the evening. (C5)
Job Perception and Job Satisfaction
Of the 14 counselors, 9 said that counseling was just a formality because they felt most of the clients counseled were not interested in listening to them. Of the 14 counselors, 5 also said that they could not provide quality counseling because the “targets” set were very high for their ICTCs. Almost all the counselors (13 of 14) said that they were insecure about their job as the posts are not permanent and that they feared being transferred or losing the job. All of them were not satisfied with the pay scale they received as it was not adequate for their qualification. Other factors that caused dissatisfaction were the lack of support (8 of 14) and having to perform more clerical duties than counseling (7 of 14). Despite the above-mentioned factors, 12 of 14 counselors agreed that they felt valued by clients and colleagues (Table 2). Only few (4 of 14) counselors said that they do not have adequate time to carry out their daily duties. As said by some of the counselors. Most of the time it is a formality. Most of them (Clients) won’t have any interest in listening to us, they come sit forcefully and go. (C2) I am working since 7 yrs. My job is still not permanent. For how long can I be in the same state? If I get a better job, I will quit. The training what they have given us will go waste. (C12) When lots of clients are waiting we won’t be in a state to lose the clients because of the target we do counseling for formality sake. (C7) Since we have done a master’s degree we cannot sit at home that is the only reason why we are working. (C6)
Problems Faced by Counselors in Providing Services
Maintaining confidentiality
All the counselors felt that they are not able to maintain confidentiality because they not only have to share the information with doctors and nurses but also with the field staff such as auxiliary nurse midwives (ANMs), link workers, and accredited social health activists (ASHA) called shared confidentiality (Table 2). This has led to the clients complaining that their status is no longer confidential. All the counselors felt that visiting clients at their residence was unethical, as the clients themselves had voiced this opinion. Issues as identified by counselors in their own words. In theory we are told not to break confidentiality but practically we are not able to do that because we have “shared confidentiality” where we have to tell others. Patients are blaming us. But we are not in a stage to answer. (C7) Shared confidentiality is truly wrong, patients tell us not to tell anyone, but our officers advise us to give the information to the ANMs, and hospital staff, but patients insist that we do not tell anyone. What to do? (C4) Lot of clients say “don’t come home because others will come to know” but the order we are given is to visit 4 to 5 other houses nearby the clients house and then go to the clients’ house. (C3) Though we have to follow the orders from the higher officials, is it not wrong to visit the clients’ home without their consent? (C14)
Administrative Issues
All the counselors felt that “targets” for counseling given to them would force them only in attaining the numbers, while not able to provide quality counseling (Table 2). Concerns raised were unnecessary counseling and testing of clients, not being able to follow guidelines due to the fact that they have to counsel and test 25 to 30 clients in a day, doctors viewing counseling as a waste of time and hence not exhibiting an interest in referring clients to ICTCs, which in turn affects numbers. What happens with targets is that it is not possible to drag each and every patient in the hospital because counseling is voluntary and should be given to those willing to listen, we say voluntary counseling and testing but if the targets are given, it cannot be voluntary. (C5) Doctors feel counseling is a waste of time but for other investigations doctors don’t mind patients spending time. When they send clients for counseling, they keep pressurizing us saying it is getting delayed so we just take the consent and send them (clients) without counseling. (C6)
Most of the counselors (11 of 14) also said they have difficulty in communicating with the officials, face a lack of support (13 of 14), need HIV-testing kits (5 of 14), and have to cope with a delay in receiving their salaries (14 of 14; Table 2).The following is the verbatim of counselor numbers 1,3 and 8. Though we have done post graduation, we do not have any respect in this field. They (higher officers) treat us like high school students. (C1) It is waste to share our problems with them (higher officers) so, we keep the problems to ourselves. (C3) Officers are at a higher position but they have to listen to their staff, then only we can work well and solve our problems but they are not willing to listen to us. (C8)
Discrimination Toward ICTCs
Most of the counselors (10 of 14) felt that there is discrimination and indifferent behavior toward them by both health care staff and the clients (Table 2). There is a lack of ownership by the doctors toward ICTC as an AIDS control program, as it is not a part of National Rural Health Mission (NRHM). Doctors and nurses fail to recognize the importance of counseling and sometimes clients presume that the counselors are HIV-positive individuals. As said by some of the counselors. Other hospital staffs treat us indifferently and they think we are different from a government organization. They also look at ICTC as a separate thing not as part of the hospital. Though HIV is related to health we feel we are treated as outsiders. (C12) Yes, I feel discriminated, because not everyone is treating us the same. People call us “HIV/AIDS people” they say “AIDS people.” Earlier it was more, but even now there is some amount of discrimination. (C7) They (doctors and nurses) feel we are there without any use. (C1)
Other Issues
The counselors expressed their concerns about spouse counseling and testing. They felt that women were always at a disadvantage. The common reasons stated by the counselors were unwillingness of the male partners to disclose their sero-positive status to the spouse; family members insisting that the wife should live with the husband despite his positive status, while the sero-positive woman inevitably has to separate from the husband. Few of the counselors’ verbatim presented below. In case where the husband is positive and the wife is negative the in-laws insist that she stays with him because he is her husband. Though we know that she is at risk, we do not have any say. (C8) Other problem with spouse testing is, when the husband is positive, and he does not reveal his status to wife or get her tested, how much ever we advise. What happens later is that the wife gets pregnant and then they come to us, we cannot do anything. (C4) The problem I am facing is when wife is positive and the husband is negative. I know that it can create problems in the family. In one instance the couple got separated within 1 month after that incidence. (C11)
Discussion
Counseling still continues to be the best intervention available and counselors have a major role to play in the prevention of HIV/AIDS. The qualitative nature of our study helped in exploring the various aspects of HIV counseling and testing services as perceived by the counselors. The factors identified by the counselors could throw light on the issues that may help in better service delivery at ICTCs. In our study, most of the counselors were females; whereas in the Egyptian 6 and South African studies, 7 male counselors outnumbered the females. The nurse counselors and social workers in cases of South African study 7 had an experience of 8 years that was almost similar to the experience of senior counselors in our study. Most of the counselors in our study were social workers trained for HIV counseling; whereas in case of South African study the counselors were nurses and community volunteers. 7
Counselors identified issues related to refresher training and expressed dissatisfaction with the training they received. This is an indication for the NGOs conducting the training and program officers, to review the structure and content of the training. There appears to be poor job perception among most of the counselors as they felt counseling was a formality. Achieving targets and disinterest among clients were the main hindering factors identified by the counselors leading to poor job perception. With respect to disinterest among the clients, a client satisfaction study conducted in the same setting showed that only 32% of the clients could recollect what was discussed during the counseling session. 9 It was also evident from the FGD that majority of the counselors were insecure about their jobs, as they were not permanent ones, contract for the same being renewed once a year, and the pay scale being based on their performance. 2 These factors in turn could affect their performance. The policy makers could consider a uniform pay scale for the counselors not based on their individual performance, as those working at low client ICTCs would receive low pay when compared to their counterparts at high client load centers.
Counselors raised concerns about shared confidentially and home visits. Shared confidentially was introduced in the NACP with the intention of improving the utilization of ICTC services. Since the information about HIV-positive clients are shared with various field workers, the chances of breaching confidentiality is very high. The authors strongly feel that field workers and health care professionals should be cautioned about maintaining strict confidentiality. Additionally, home visits by counselors makes maintaining confidentiality difficult for the clients. These 2 issues must be treated as very sensitive, as they could affect the clients and hence the utilization of ICTC services.
The views of counselors also suggest that there is lack of ownership among doctors and nurses toward ICTCs. Currently, all national programs in India such as Revised Tuberculosis Programme, Reproductive Child Health (RCH), National Leprosy control Programme, and so on are integrated under National Rural Health Mission 10 except for NACP III. This could be one of the reasons why doctors and nurses treat ICTCs as an additional responsibility and lack ownership.
“Targets” for counseling for ICTCs is fixed under the program to improve utilization of services at the ICTCs and also is the basis for assessing counselor’s performance. But according to the counselors, these targets are affecting the quality of services provided. This could be because at centers with high client load counselors have to counsel more clients, whereas in low client load centers counselors have to search for clients to achieve the numbers. These factors could affect the quality of counseling provided at ICTCs. Hence, authors suggest that a “target-free approach” for HIV counseling could be considered. The study was conducted among small group of counselors in a district of South India, which is one of the limitations of our study.
Footnotes
Acknowledgments
The authors would like to thank Dr Shashi S Associate Professor Department of Community Medicine KMC, Manipal and Dr. Ashok, District AIDS control officer of Udupi District for their valuable inputs during the study and all the counselors who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.