
Abstract
Studies of sexual behavior among HIV-infected Thai youth show conflicting results due to the different ages of the respondents. This study examined the relationships between sexual self-efficacy and risk behaviors among 92 HIV-positive Thai youth aged 14 to 21 years. A questionnaire previously validated in Thailand measured sexual self-efficacy. There were low levels of sexual activity with 13 respondents having sex in the last 6 months. The sexual self-efficacy scales were inversely related to the risk behaviors of having sex, having multiple partners, and drinking alcohol in the last 6 months. The scores of the sexual self-efficacy scale and its subscales were significantly lower in those aged 17 to 21 than in 14 to 16. Sexual risk behaviors were significantly higher in those aged 17 to 21 than in 14 to 16. These findings suggest that interventions to increase sexual self-efficacy should be emphasized as HIV-infected Thai youth reach late adolescence.
Introduction
Thailand instituted routine, voluntary HIV testing during pregnancy, beginning in 1991. 1 Because of this HIV testing during pregnancy even before treatment was available, Thai clinicians were able to identify a significant number of newborns who were HIV infected. After highly active antiretroviral therapy became available, treatment was given to these children. 2 As a result there are a significant number of young Thais who are reaching the ages when they are likely to be sexually active. Because of their potential to spread HIV infection, they become an important target for preventive action. This must be done in the context of the level of sexual risk behaviors in which young, HIV-infected youth are engaging.
The literature on these behaviors is conflicting. Lee and Oberdorfer 3 conducted a study in 2007 to 2008 in Northern Thailand of young HIV-infected persons and found that only a small proportion of them were engaging in high-risk behavior. Other researchers who conducted studies of HIV-infected youth in Northern Thailand in the late 1990s and early 2000s found that youth living with HIV/AIDS engaged in risky sexual behaviors including a high rate of sexual activity, low levels of condom use, having multiple partners, and alcohol consumption. 4 –7 Similar high-risk behaviors were found more recently by Settheekul et al. 8
The different results in these studies might be due to a number of factors. The Lee and Oberdorfer study was conducted on relatively young adolescents with a median age of 14.6 years. This is below the usual age of sexual debut of adolescents in Northern Thailand, which was found in one study to be a median of 17 years for men and 18 years for women. 9 The early studies of risk behaviors of HIV-infected youth were done on a mixture of perinatally infected and behaviorally infected young persons. Also, the early studies were directed toward individuals who were relatively recent entrants to HIV treatment that provides health education and counseling.
The differences in sexual behavior between the 2007 to 2008 study and the earlier studies may be due to the fact that perinatally infected youth have been in regular contact with the health care system for many years and receive education and counseling about how to avoid unsafe sexual behaviors. This may have increased their capability to manage potentially dangerous sexual encounters. This ability has been termed self-efficacy that was defined by Bandura as “self-belief in one’s capability to exercise personal control” and is concerned with the individuals’ beliefs that they can exert control over their motivation and behaviors. 10 Previous studies of HIV risk behavior have shown that high self-efficacy is associated with higher levels of condom use. 11 Moreover, the self-efficacy in condom use was related to gender, negotiating skills, knowing how to avoid sexual encounters and managing depressive symptoms. 12 –16 Other studies showed that lower sexual risk taking among youth was associated with high sexual self-efficacy such as resistive efficacy or the confidence to refuse unwanted or unsafe sexual situations. 17 –19 Therefore, it seems that sexual self-efficacy among youth living with HIV/AIDS has an important protective effect against HIV transmission and may account for the low level of sexual activity observed by Lee and Oberdorfer. 3 However, little is known about factors related to sexual self-efficacy among Thai youth living with HIV/AIDS.
Therefore, a study was conducted to assess the relationships between sexual self-efficacy and related factors, respondent characteristics and sexual risk behaviors among youth living with HIV/AIDS in Thailand. The study also included individuals up to 21 years to see whether there were changes in the sexual behaviors and self-efficacy of HIV-infected Thai youth as they grow older.
Methods
After obtaining approval from the Institutional Review Board of the Faculty of Nursing of Chiang Mai University, the researchers established relationships with the network of people living with HIV/AIDS, which operates out of 4 community hospitals in Chiang Mai province. Potential participants were directly contacted by the researchers and they were asked to refer others to the study. The inclusion criteria were that the participants were between 14 and 21 years of age, were diagnosed as being HIV sero-positive, and were sufficiently literate in the Thai language to complete the questionnaires. Data were collected in July to October 2011. Ninety-two youth agreed to participate in the study.
Instruments
The instruments included a demographic data and sexual behavior form which was used to obtain information about gender, age, religion, educational background, items related to HIV status including the length of time since knowing their status and presumed route of HIV infection. This portion of the questionnaire also inquired about sexual risk behaviors such as having sexual intercourse, having multiple partners, condom use, and alcohol consumption. The second part of the questionnaire was the Sexual Self-Efficacy Questionnaire (SSEQ) that was modified from the Sexual Self-efficacy scale of Srisuriyawet. 19 The 20-item SSEQ consisted of 4 scenarios, each scenario having 5 questions dealing with (a) self-efficacy for refusing sex; (b) self-efficacy for bringing up the issue of condoms in conversation; (c) self-efficacy for convincing one’s partner to be safe, even if the partner said he or she hated condoms; (d) self-efficacy for convincing one’s partner to be safe, even though both hated condoms; and (e) self-efficacy for refusing sexual intercourse, if the partner would not be safe. Of the 20 items, 16 addressed safe sex self-efficacy and 4 addressed refusal sex self-efficacy. In each item, the respondents were asked to indicate how confident they were about engaging in each behavior ranged from 0 to 10. A total score, for the safe sex self-efficacy component of the instrument, had a possible range of 0 to 160, which was obtained by summing the response scores across the 16 relevant items. Higher scores indicated a higher self-efficacy to have safe sex. A total score, for the refusal sex self-efficacy component of the instrument, has a possible range of 0 to 40, which was obtained by summing the response scores across the 4 relevant items. Higher scores indicated a higher self-efficacy for refusing sex. For this study, Cronbach α coefficient were .98 for the overall 20-item SSEQ, .99 for safe sex self-efficacy subscale, and .86 for refusal sex self-efficacy subscale.
Data Analysis
Descriptive statistics were used for the demographic data. The relationships between sexual self-efficacy and related factors (respondent characteristics and sexual risk behaviors) were examined using Pearson correlation, Spearman correlation, independent t test, and logistic regression analysis.
Results
The sample consisted of 58 males (63.0%) and 34 females (37.0%) aged between 14 and 21 years (mean= 15.96, median = 16.0). Nearly three-fourths (73.0%) were Buddhist and most of them had attended high school (84.8%). Causes of HIV infection were mother to child (93.4%), sexual behavior (3.3%), did not know (2.2%), and blood transfusion (1.1%). The majority of the respondents (70.7%) reported that they had known that they were HIV positive for more than 7 years suggesting that most had known of their status before reaching puberty. With regard to risk behaviors, 27.2% reported drinking alcohol in the last 6 months. Thirteen respondents (14.1%) had sex in the last 6 months and 7 (7.6%) of these had multiple partners. Sixty-eight of the respondents (73.9%) reported that they had never had sex. Of the 24 youth who reported having ever had sex, 3 said that they always used condoms during sex and 7 said that they used them sometimes while 14 said that they never used condoms (Table 1).
Respondent Characteristics and Their Sexual Risk Behaviors.a

Abbreviation: SD, standard deviation.
aN = 92.
Table 2 shows the correlations between sexual self-efficacy scale or its subscales and the respondents’ characteristics. There were no statistically significant differences between sexual self-efficacy, its subscales and gender, educational background, the length of time since knowing their status, and cause of HIV infection. There was significant inverse relationship between age and refusal of sex efficacy subscale. Sexual experience in the last 6 months, having multiple partners, and drinking alcohol were negatively correlated with the overall efficacy scale and both of its 2 subscales. There was no relationship between the scales and condom use.
Correlation Between Sexual Self-Efficacy and Respondent Characteristics and Risk Behaviors.
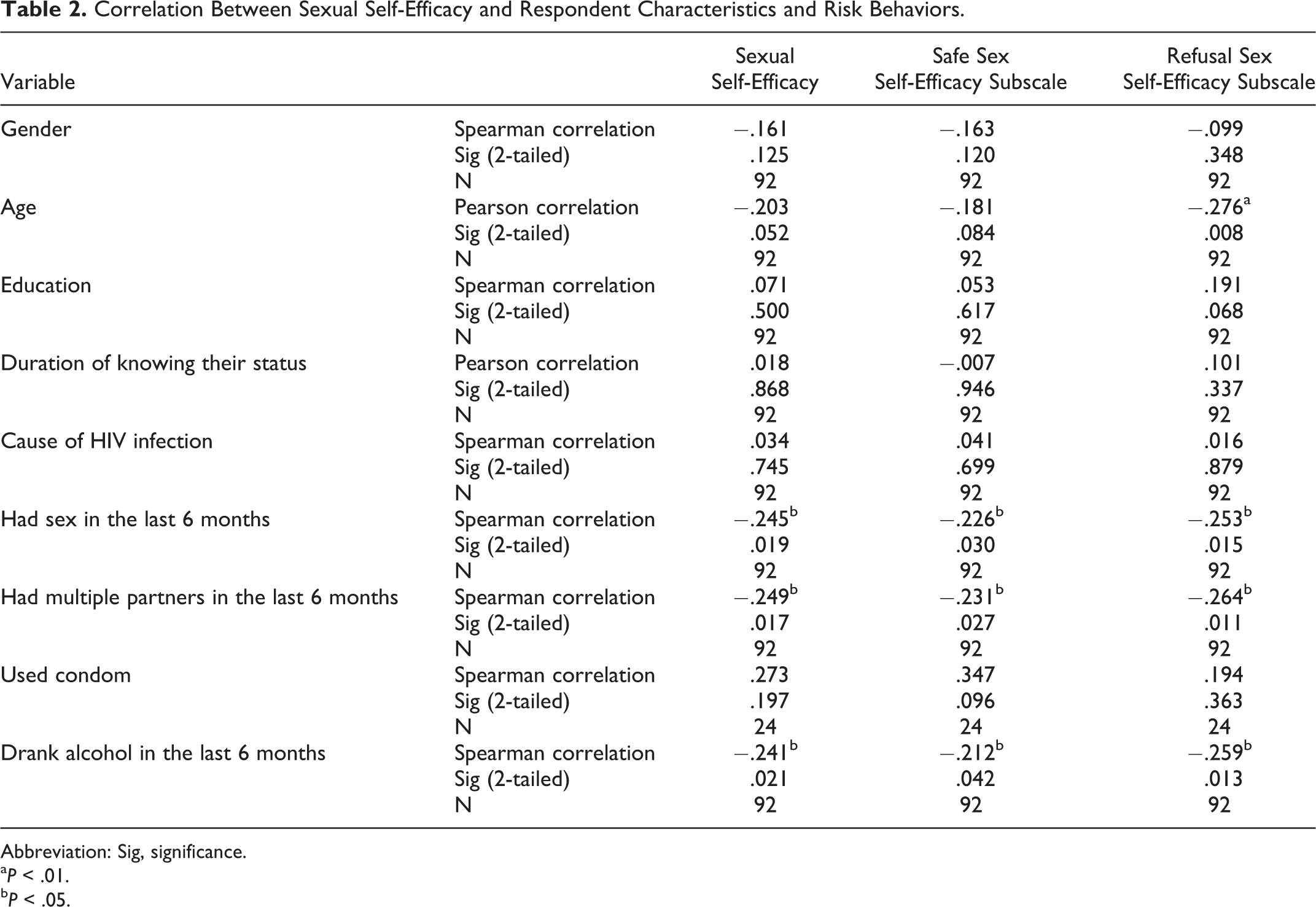
Abbreviation: Sig, significance.
a P < .01.
b P < .05.
Youth aged 14 to 16 were less likely to have had sex in the last 6 months, to have had multiple partners, and to have drunk alcohol than those aged 17 to 21. Only 3 younger persons (4.9%) had sex in the previous 6 months, while 32.3% of the 17 to 21 years old had done so. Only 1 of 14 to 16 years old had more than 1 sexual partner, while 6 respondents from the older group had multiple partners. Alcohol use in the younger group was also lower than that in the older group (14.8% vs. 51.6%). The overall self-efficacy score was 132 for the younger group and 117 for the older group (P = .025). The younger group’s safe sex efficacy scale score (105) and the sex refusal scale (27) were both higher than the older group’s scores of 94 and 22, respectively. These differences were significant for the self-efficacy scale at P = .045 and for the sex refusal scale at P = .000.
Table 3 shows the relationship between sexual self-efficacy and risk behaviors when controlling for age and gender. It revealed that sexual experience in the last 6 months and having multiple partners were negatively correlated with the overall efficacy scale and both of its 2 subscales.
The Relationship Between Sexual Self-Efficacy and Risk Behaviors with Control for Age and Sex.

Abbreviation: Sig, significance.
aN = 92.
b P < .05.
Table 4 shows logistic regression analysis with age, gender, education, and sexual self-efficacy on risk behaviors. It shows that sexual self-efficacy and age are related to risk behaviors. Higher sexual self-efficacy scores are associated with not having sex and not having multiple sexual partners. Age was negatively correlated with risk behaviors with increasing age being associated with having had sex in the last 6 months, having multiple sexual partners, and drinking alcohol.
Logistic Regression Analysis with Age, Gender, Education, and Sexual Self-Efficacy on Risk Behaviors.a

Abbreviation: CI, confidence interval; LL, log likelihood; SE, standard error.
aN = 92.
b P < .01.
c P < .05.
Discussion
The results revealed that youth living with HIV/AIDS were not very likely to have engaged in sexual risk behaviors, with 73.9% having never had sex and only 14.1% having sex in the last 6 months. These findings are consistent with the findings of Lee and Oberdorfer which found low rates of sexual activity in younger (median age of 14.6 years) HIV-infected youth. 3 The study also showed that there are declines in the self-efficacy score as HIV-infected youth become older than 16. This may be due to the fact that younger persons have not had experience with the situations depicted in the scenarios and are responding to hypothetical situations while the older group has had to deal with actual situations and are less confident of their ability to manage sexual encounters. This is borne out by the fact that age continues to have an important impact when other variables are included in a multivariate analysis. The results also suggest that young people have received the knowledge of what must be done to avoid HIV transmission. However, the knowledge of how to control and manage sexual situations seems to be lacking and becomes apparent when one reaches an age of actually having to deal with these issues. This means that factual education seems to be working but that behavioral education must be instituted as HIV-infected youth transition from early to late adolescence. The scenarios used in this study were easily understood by the youth in this study. Education based on these or similar scenarios could be used to teach about how to manage sexual risks and encounters. The scenarios used in this study were understood and provided a data collection method to which the youth in this study could easily respond. Education based on these or similar scenarios could be used to teach about how to manage sexual risks and encounters. Given that nearly 60% of the sexually active respondents said that they never used a condom, the negotiation of condom use should be an important component of such education programs.
Conclusion
This study has a number of limitations. Only 92 HIV-positive Thai youth in 1 location of Thailand were used to obtain the data. Thus, the results cannot be generalized to other populations. In addition, the respondents may not have fully expressed their true sexual behaviors and sexual self-efficacy since sexual issues are very sensitive topics in Thai society and are compounded by the HIV status of the respondents. The instrument that was used to create the self-efficacy scales only measured the respondents’ reactions to scenarios and may not reflect actual behaviors in the real world. However, it is important to note that the lower self-efficacy scales were associated with risky sex behaviors. This suggests the scale is measuring aspects of what it was intended to measure. This provides evidence that other researchers can use the approach of using scenarios to measure self-efficacy in managing sexual encounters in different populations of HIV-infected and uninfected persons.
Footnotes
Acknowledgments
The authors would like to thank the Thai youth living with HIV/AIDS who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to thank the National Research University Project under Thailand's Office of the Higher Education Commission for financial support (WF62). This publication resulted (in part) from research supported by the Baylor-UTHouston Center for AIDS Research (CFAR), an NIH-funded program (AI036211).