
Abstract
Mycobacterium sherrisii was first described as a novel species in 2004 but recently has begun to be more formally recognized with the use of new sequencing techniques. There have only been about 10 cases reported internationally, and we report the first case of M sherrisii in the United States. The mycobacterium was isolated from acid-fast bacilli cultures of a specimen obtained from a bronchoalveolar lavage and blood in a newly diagnosed HIV-infected, US-born patient presenting with sepsis. The patient was started on streptomycin, ethambutol, azithromycin, and rifampin with an improved clinical course. This report indicates the clinical presentation along with the varying drug susceptibilities to the emerging M sherrisii.
Keywords
Introduction
Mycobacterium sherrisii was first described and proposed as a novel group of atypical mycobacterium related to Mycobacterium simian in 2004 by Selvarangan et al. 1 A more recent study further defined its phylogenetic position and proposed the formal recognition of M sherrisii with type strain 4773T (=ATCC BAA-832T=DSM 45441T). 2 There have been 8 reported cases of this new strain, mostly occurring in Africa, and mainly in HIV-infected patients with a severely immunocompromised state. Only 1 case of pulmonary M sherrisii has been reported in a non-HIV-infected patient. 3 Due to its recent recognition and close resemblance to M simiae, the clinical features of patients infected with disseminated M sherrisii are not yet known nor has the proper treatment with varied drug susceptibilities and clinical results been established.
Case Report
A 48-year-old African American male born and raised in the United States was diagnosed with HIV and presumed Mycobacterium avium-intracellulare infection in February 2012. Initial absolute CD4 count was 2 cells/mm3 with HIV RNA quantitative >1million copies/mL. The patient started on clarithromycin, ethambutol, prednisone, and Bactrim DS with instructions to follow up at an HIV clinic for starting antiretroviral (ARV) medication. In May 2012, he was started on efavirenz (EFV), abacavir (ABC), and lamivudine (3TC). Three weeks later, he developed diarrhea, nausea, vomiting, and shortness of breath. His caseworker noticed increased confusion upon speaking with him on the telephone and recommended that he go to the emergency room. On physical examination, there were diminished lung sounds bilaterally with a regular tachycardia. He was disoriented to place but able to state name and date. No palpable lymph nodes or hepatosplenomegaly were evident. Neurodermatitis was present on bilateral arms, chest, and back. Over the next 24 hours, he became febrile, tachycardic, and hypotensive. Initial laboratory tests indicated acute renal insufficiency with an estimated glomerular filtration rate of 6, anion gap metabolic acidosis, and normocytic anemia. Computed tomography of the chest indicated right middle lobe and lower lobe opacities along with multiple enlarged portal, celiac, mesenteric, and retroperitoneal lymph nodes. Prior records were reviewed and bronchoalveolar lavage from previous hospitalization indicated an atypical mycobacterium most closely related to M simiae. The 16S ribosomal RNA sequencing was then performed to differentiate it from other atypical mycobacterium. Acid-fast bacilli blood cultures were also obtained and indicated M sherrisii. The patient underwent hemodialysis, which improved his mental status. Initial broad-spectrum antibiotics of vancomycin/cefepime were stopped, and he was placed on intramuscular streptomycin, intravenous azithromycin, oral ethambutol, and intravenous rifampin. The ARV medications were restarted (EFV, ABC, and 3TC). Repeat CD4 absolute count elevated to 40 cells/mm3 and HIV RNA quantitative decreased to 153 copies/mL. Susceptibilities from both the blood and the sputum samples are listed. Streptomycin, ethambutol, azithromycin, and rifampin were started, and the patient clinically improved, so the medications were administered for 2 weeks, and then clarithromycin and ethambutol were orally continued.
Discussion
Newer technology has resulted in a novel species of mycobacterium differentiated from the atypical mycobacterium group. With the gene sequencing technique, the identification of M sherrisii can be performed, but its clinical significance is yet to be determined. It is probable that many high-performance liquid chromatography methods have designated this new species as M simiae or labeled it as a member of the Simiae-Avium group. Further investigation will need to be done in regard to the clinical outcomes with varying drug combinations and approaches.
Conclusion
The newly designated species of mycobacterium, M sherrisii, has been shown to cause infection in HIV-infected individuals. The few cases reported have mostly been from Africa4–6 with 1 validated species in Thailand 7 and most recently a reported case in Singapore. 8 We report the first case of disseminated M sherrisii in the United States. The clinical features have varied from case to case, with some isolated pulmonary disease as well as disseminated disease. Our patient originally presented with respiratory symptoms that, after shortened therapy with clarithromycin, ethambutol, and prednisone due to noncompliance, further progressed into acute renal insufficiency and septic shock. The clinical response to treatment has varied across all the cases, along with drug susceptibilities described. Further characteristics of M sherrisii and its clinical significance will need to continue to be reported, as more cases are identified throughout the world.
Drug Susceptibilities.
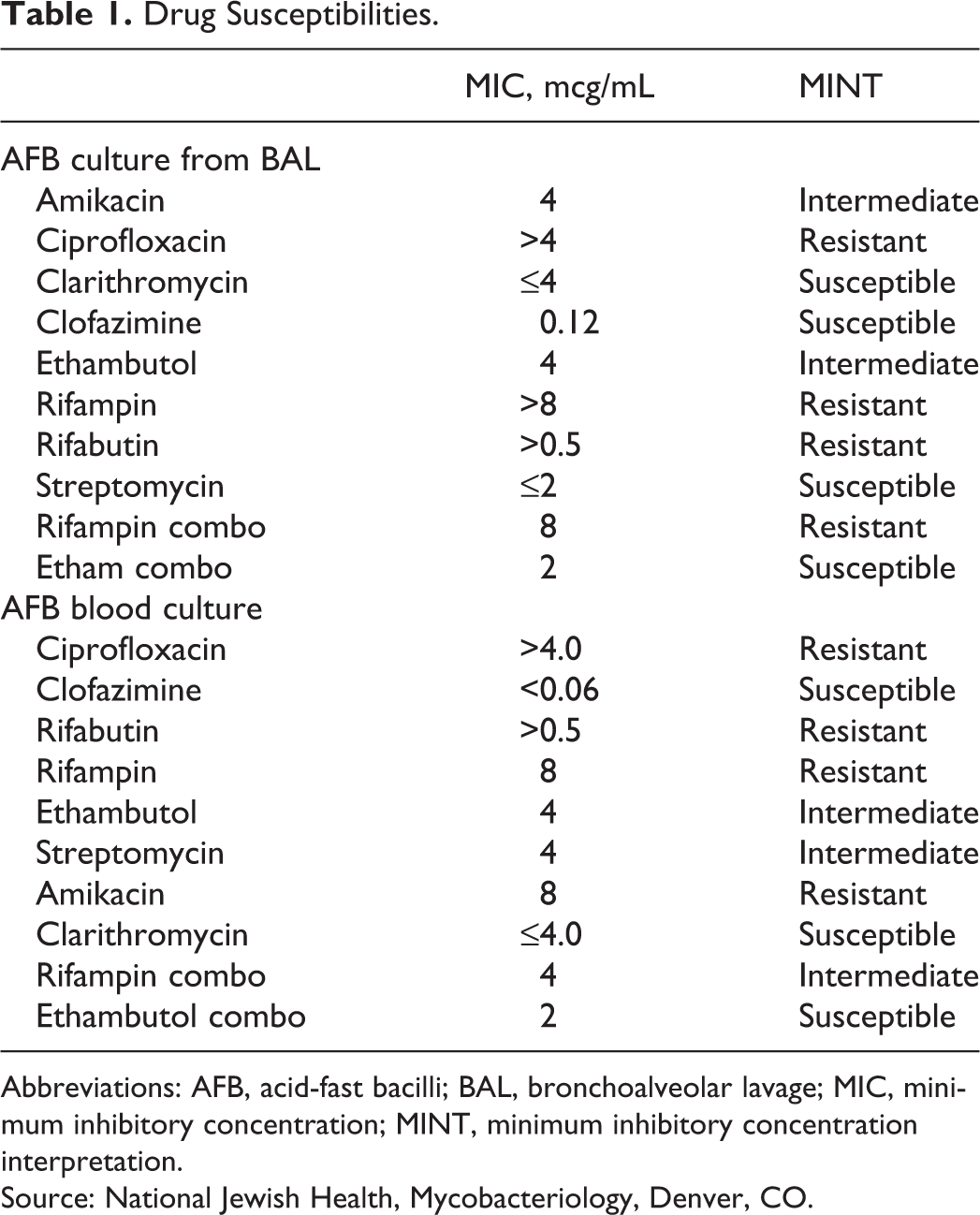
Abbreviations: AFB, acid-fast bacilli; BAL, bronchoalveolar lavage; MIC, minimum inhibitory concentration; MINT, minimum inhibitory concentration interpretation.
Source: National Jewish Health, Mycobacteriology, Denver, CO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.