
Abstract
Studies have shown immunological and morphological alterations in the esophagus during the course of AIDS. Esophageal postmortem samples of 22 men with AIDS autopsied in a teaching hospital between 1982 and 2009 were collected. We carried out revision of the autopsy reports and medical records, morphometric analysis (Image J and KS-300 Kontron-Zeiss), and immunohistochemical (anti-S100, anti-IgA, anti-IgG, and anti-IgM) analysis of the esophagus. In accordance with most of the parameters evaluated, age and the smoking habit harmed the esophageal local immunity, whereas the use of antiretroviral therapy improved the immune characteristics of this organ. Patients with esophagitis also presented immunological fragility of the esophagus. This leads to the conclusion that alterations in the esophageal epithelium of patients with AIDS are not only caused by direct action of HIV but also the clinical and behavioral characteristics of the patient.
Introduction
AIDS is a dynamic and unstable global phenomenon that progresses in multiple dimensions and is going through important epidemiological changes. 1 One of the phenomena of the AIDS pandemic is the arising of a new vulnerable population, the elderly. 2 Several cohort studies have shown that older patients have faster progression to AIDS than younger patients, 3,4 and that the survival time after an infection by AIDS is significantly lower in patients older than 50 years. 5,6 Moreover, individuals going through the aging process present a worse evolution of opportunistic infections when compared with younger individuals. 7
In the early years of the pandemic, the follow-up of patients with AIDS was limited to the treatment or control of opportunistic infections. 8 From 1997 onward, due to the global introduction of the highly active antiretroviral therapy (HAART), a progressive decrease in mortality and incidence of opportunistic infections was noticed. 9 However, very little is known about the influence of this therapy on the local immunity of the esophagus.
Besides alterations in the epidemiologic profile of AIDS, some habits may influence the prognosis of these patients. The smoking habit, for example, may exacerbate possible alterations in the local immunity of the esophagus of patients with AIDS. Tobacco and its derivatives may induce several alterations in the immunological system, particularly in the natural killer cells and Langerhans cells (LCs). 10,11 Alterations in these cells suggest a local immunodeficiency. 12
The local immunity of the esophagus may be evaluated through the analysis of the esophageal epithelium, since the epithelial cells constitute a physical barrier, vital to the defense against pathogens. 13 Moreover, the LCs found in this epithelium are important to the cellular immune surveillance system, as they are antigen-presenting cells and activate particularly the CD4 T lymphocytes. 14,12 Another relevant factor to be evaluated is the expression of antibodies in the mucosas, since they may constitute the first line of immune defense against infections. 15
Studies investigating the esophagus of patients with AIDS have suggested a decrease in the local immunity of this organ. 16,17 The aim of this study was to evaluate the influence of clinical and behavioral characteristics, such as age, smoking, antiretroviral therapy (ART), and esophagitis on the morphology and immunity of the esophageal epithelium and on the viral load and CD4 T lymphocyte count in male patients with AIDS.
Material and Methods
This study was approved by the Triângulo Mineiro Federal University Research Ethics Committee on August 6, 2007, approval number 902.
Previous studies demonstrated the influence of gender on the local immunity of the esophageal epithelium. 17 In order to avoid hormonal variations caused by the menstrual cycle, only men were included in this study. Postmortem samples removed from the upper third of the esophagus of 22 male individuals with AIDS, aged 21 to 51 years, autopsied in the General Pathology Division of General Hospital of Triângulo Mineiro Federal University, in the state of Minas Gerais, Brazil, were collected from 1982 to 2009.
AIDS diagnosis was confirmed by evidence of at least one AIDS-defining disease presented by the patient and by CD4 T lymphocyte count below 200 cells/mm3. 18 All the patients with AIDS observed in this study died of infection during the post-HAART era. 19 However, not all of them had made use of the therapy, which may be explained by the fact that many of them looked for health services in an advanced stage of the disease.
The esophagi observed in this study were recovered from an archive in the General Pathology Division and were transversally sectioned where the epithelium was preserved. The samples were grouped according to treatment with ART: men who were receiving ART (n = 9) and men who had never received ART (n = 13); according to smoking habits: smokers (n = 13) and nonsmokers (n = 9); and according to esophagitis: patients without esophagitis (n = 14) and patients with esophagitis (n = 8).
The cases concerning incomplete autopsy reports, or men who had some diseases that affect the morphology of the esophagus, such as megaesophagus caused by Chagas’ disease, alcoholism, and gastroesophageal reflux, were excluded. It can explain the small number of patients used in this study. Information relating to date of diagnosis, treatment with ART, smoking habits, values of the last viral load examination, and CD4 T lymphocyte count (0 to 3 months before the date of death) were collected from the clinical record, whereas age and any alterations in the patients’ esophagi were collected from the autopsy reports. The fragments were subjected to histological processing, and then 4-µm-thick serial sections were cut for histochemistry and immunohistochemistry procedures.
Hematoxylin and eosin staining was carried out so as to provide morphometric analysis of the thickness, number of layers, and average cell diameter of the esophageal epithelium (Figure 1). For the morphometric analysis, images of the fields were captured by a video camera coupled to a light microscope. Image J 1.32j Program (National Institutes of Health, USA; http://rsb.info.nih.gov/ij/), an interactive analysis system, was used to measure the thickness. The whole esophageal epithelium was measured by tracing 5 straight lines on different parts of each field to be analyzed. 16,17 Below each line, the nuclei of the cells were counted in order to determine the number of cell layers in the epithelium. The cell’s average diameter was obtained by dividing the thickness by the number of nuclei in each measure.

Thickness, number of cellular layers, and mean cellular diameter (A; HE, ×320); immunostaining of Langerhans cells (B; anti-S100, ×620); and immunostaining of IgA, IgG, and IgM (C, D, and E; anti-IgA, anti-IgG, and anti-IgM, respectively, ×320) in the esophageal epithelium of male patients with AIDS.
Immunostaining of LCs, immunoglobulin A (IgA), IgG, and IgM was performed, respectively, with anti-S100, anti-IgA, anti-IgG, and anti-IgM (DAKO, Denmark S/A) in the concentrations of 1/400, 1/1000, 1/1000, and 1/800, respectively. The antigen retrieval was carried out with sodium citrate buffer for LCs, whereas trypsin buffer was used for IgA, IgG, and IgM. All antibodies were incubated for 2 hours; LSAB+System-HRP (DAKO) was used in the process of revelation; and diaminobenzidine was used as substrate chromogen (Figure 1).
The LCs positively stained by immunohistochemistry were counted in the whole extension of the esophageal epithelium and expressed as number of cells per area (mm2). The total number of LCs was determined in each field.
The quantification of IgA, IgG, and IgM, positively stained by immunohistochemistry, was performed by Kontron KS-300 (v.2.0, Carl Zeiss) system, and the results were expressed in percentage values in each field.
Statistical analysis was performed using SigmaStat 2.03 software. In variables with normal distribution and similar variances Student t test was used, and the results were expressed in mean ± standard deviation; otherwise, Mann-Whitney test (T) was used and the results were expressed in median (minimum– maximum). Correlation between the 2 variables with normal and not normal distribution was analyzed by Pearson coefficient (r) and Spearman rho coefficient (rS) test, respectively. The difference of P < .05 was regarded as statistically significant.
Results
Age
The age of the patients correlated negatively and significantly with the thickness of the epithelium (rS = −0.168; P < .01), the number of epithelial cell layers (rS = −0.130; P < .01), the mean diameter of the epithelial cells (rS = −0.124; P < .01), the number of LCs (rS = −0.271; P < .01), and the expression of IgA (rS = −0.123; P = .0016), IgG (rS = −0.386; P < .01), and IgM (rS = −0.351; P < .01) in the esophageal epithelium.
Use of ART
Among the 22 patients observed, 9 (40.90%) were undergoing ART, and the therapy time varied from 1 to 10 years. Fifteen (68.18%) died after a year or less of the diagnosis, though 13 (86.66%) of the patients were not receiving ART. On the other hand, 7 (31.81%) patients receiving ART survived for 3 to 14 years after the diagnosis.
Patients receiving ART presented with significantly lower thickness of the esophageal epithelium, lower number of epithelial cell layers, and lower IgA expression, and the number of LCs and IgG and IgM expression were significantly higher than the patients who were not receiving ART (Table 1).
Thickness of the Epithelium (µm), Number of Epithelial Cell Layers, Mean Cellular Diameter of the Epithelial Cells (µm), Number of Langerhans Cells (cells/mm2), and Expression of IgA, IgG, and IgM (%) in the Esophageal Epithelium of Male Patients with AIDS Who Had Never Received ART and Who Were Receiving ART.

Abbreviations: ART: antiretroviral therapy; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; Max, maximum; Med, median; Min, minimum; T, Mann-Whitney test.
a T = 1 974 090.000, P < .001.
b T = 1 956 562.000, P < .001.
c T = 2 093 733.000, P= .958.
d T = 105 765.500, P = .935.
e T = 80 968.500, P < .001.
f T = 97 477.500, P < .001.
g T = 97 415.500, P < .001.
The treatment time of the ART correlated negatively and significantly with the number of epithelial cell layers (r S = −0.0596; P = .0289) and positively and significantly with the number of LCs (r S = 0.118; P = .0416) and IgA expression (r S = 0.240; P < .01) in the esophageal epithelium. A positive, though not significant, correlation was observed between the treatment time of the ART and the mean diameter of the epithelial cells and the expression of IgG and IgM, whereas treatment time of the ART correlated negatively, though not significantly, with the epithelial thickness.
Smoking
According to data collected from the patients’ medical records, 13 (59.09%) were smokers, and the duration of smoking varied from 1.5 to 40 years. The smokers presented significantly larger epithelial thickness and mean cell diameter, and a higher number of LCs, and expressison of IgA, IgG, and IgM in the esophageal epithelium was significantly smaller than the nonsmokers (Table 2).
Thickness of the Epithelium (µm), Number of Epithelial Cell Layers, Mean Cellular Diameter of the Epithelial Cells (µm), Number of Langerhans Cells (LCs; cells/mm2), and Expression of IgA, IgG, and IgM (%) in the Esophageal Epithelium of Smoking and Nonsmoking Male Patients with AIDS.

Abbreviations: IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; Max, maximum; Med, median; Min, minimum; T, Mann-Whitney test.
a T = 1 189 154.500, P < .001.
b T = 1 507 530.000, P = .812.
c T = 1 164 782.000, P < .001.
d T = 110 009.000, P = .058.
e T = 106 543.500, P < .001.
f T = 95 477.500, P = .008.
g T = 99 139.500, P < .001.
A negative and significant correlation was observed between the duration of smoking and the epithelial thickness (r S = −0.131, P < .01), the number of epithelial cell layers (r S = −0.295, P < .01), the number of LCs (r S = −0.394, P < .01), and the expression of IgG (r S = −0.288, P < .01) and IgM (r S = −0.189, P = 0.0018) in the esophageal epithelium. On the other hand, a positive and significant correlation was observed between the duration of smoking and the mean diameter of the epithelial cells (r S = 0.0596, P = .0272) and the expression of IgA (r S = 0.217, P < .01).
Esophagitis
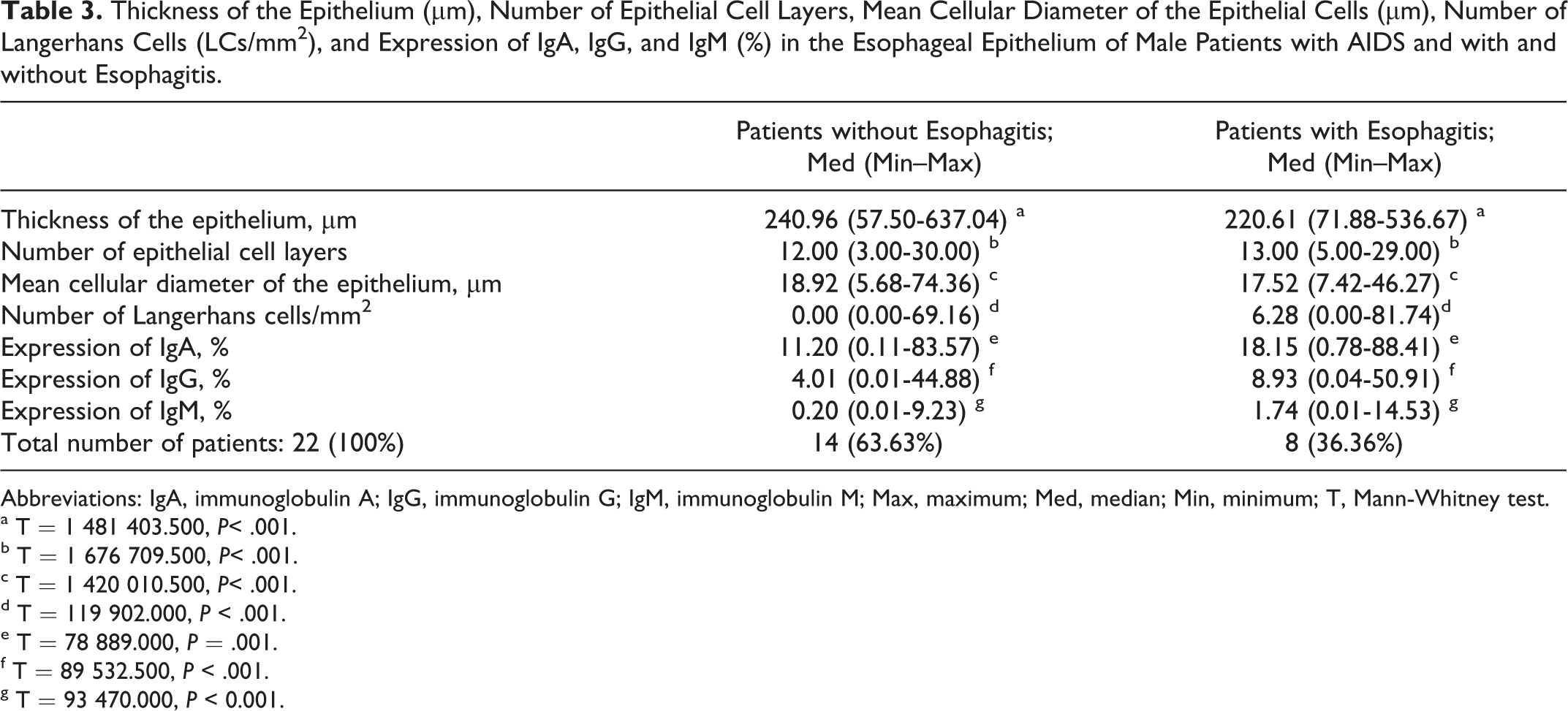
According to data in the autopsy reports, 8 (36.36%) of the 22 patients had esophagitis. Candida albicans was identified as the etiologic agent in 5 of them, whereas the etiology of the 3 other cases was not identified. As for the analysis carried out, the patients with esophagitis presented epithelial thickness and mean cell diameter significantly smaller and the number of epithelial cell layers, number of LCs, and expression of IgA, IgG, and IgM significantly higher than the patients without esophagitis (Table 3).
Thickness of the Epithelium (µm), Number of Epithelial Cell Layers, Mean Cellular Diameter of the Epithelial Cells (µm), Number of Langerhans Cells (LCs/mm2), and Expression of IgA, IgG, and IgM (%) in the Esophageal Epithelium of Male Patients with AIDS and with and without Esophagitis.
Abbreviations: IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; Max, maximum; Med, median; Min, minimum; T, Mann-Whitney test.
a T = 1 481 403.500, P< .001.
b T = 1 676 709.500, P< .001.
c T = 1 420 010.500, P< .001.
d T = 119 902.000, P < .001.
e T = 78 889.000, P = .001.
f T = 89 532.500, P < .001.
g T = 93 470.000, P < 0.001.
Viral Load and CD4 T Cell Count
The viral load values of 14 of the 22 patients observed were recovered, and they ranged from 46 743 to >500 000 copies/mL. All 22 (100%) patients presented CD4 T lymphocyte count varying from 2 to 109 cells/mm3, indicating AIDS.
Younger patients of 21 to 35 years old presented higher levels of viral load and lower CD4 T lymphocyte count when compared with older patients of 36 to 51 years old. Smokers had higher levels of viral load and lower CD4 T lymphocyte count compared with nonsmokers. As for the use of ART, patients undergoing the therapy presented lower levels of viral load and higher CD4 T lymphocyte count. Patients with esophagitis presented higher levels of viral load and lower CD4 T lymphocyte count (Table 4).
Influence of Age, Tabagism, ART, and Esophagitis on the Viral Load and CD4 T Lymphocyte Count of Male Patients with AIDS.

Abbreviations: ART: antiretroviral therapy; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; Max, maximum; Med, median; Min, minimum; SD, standard deviation; T, Mann-Whitney test; t, t test.
a t = −0.273, P = .790.
b T = 101.000, P = .373.
c t = 0.894, P = .389.
d t = −0.470, P = .644.
e t = 1.694, P = .116.
f t = 0.323, P = .750.
g t = 0.725, P = .482.
h T = 103.500, P = .453.
Discussion
The tissues change gradually with age, whereby a great part of these changes is connected with the aging process. 20 The decrease in the epithelial thickness, the number of layers, and the cell diameter of the esophageal epithelium with aging may be associated with the reduction in testosterone levels in men as they get older, since one of the functions of this hormone is to increase the epithelial thickness. 21
In the current study, we observed that the older the patients were, the lower was the number of LCs and Igs expression in the esophageal epithelium. These data are in accordance with the results of the studies that demonstrated that with age there is a functional impairment of several organs and systems, and the immune system is no exception. 22 During the aging, alterations occur in the expression of functionally important cellular receptors, decrease of polymorphonuclear leukocyte population and a quantitative and qualitative reduction of the ability to produce antibodies, factors which lead to immune dysfunction. 23,24
The fact that most of the patients who died after a year or less after the diagnosis were not undergoing ART accords with the literature, which demonstrated that since November 1997, when HAART became available for all Brazilian patients with AIDS, there was a 38% decrease in mortality rates. 25,19 Therefore, the nonutilization of ART led to the premature death of the patients observed in this study.
The epithelial thickness and the number of epithelial cell layers in the esophagus were reduced in patients undergoing ART. Moreover, the longer the treatment was, the smaller was the number of epithelial cell layers. The use of therapeutic combinations containing drugs of the protease inhibitors class provided an important and sustained suppression of the viral replication, 26 increasing survival and improving the quality of life of patients living with HIV sero-positive. 27 However, long-term treatments with drug combinations may produce toxic effects. 28 The reduction in the epithelial thickness caused by the reduction in cells in the epithelium could possibly be a consequence of the therapy toxicity.
Patients undergoing ART presented a higher number of LCs in the esophageal epithelium. Also, the longer the treatment, the higher the number of LCs in the esophageal epithelium. In the course of an infection by HIV, there is a decrease in the local immunity of the esophageal mucosa due to the reduction in the number of cells connected with immune response, such as LCs. 14,16,17 Data collected during this study reinforce that ART contributes to the immune recovery of the esophagus, increasing the LC population in the epithelium.
Together with a profound immunodeficiency of T lymphocytes, HIV induces an activation and dysfunction of B lymphocytes, resulting in hypergammaglobulinemia. 29 The ART improves the status of activation and differentiation of B lymphocytes, restoring these cells’ ability to respond to the dependent activation of T lymphocytes. 30 Studies demonstrate that serum Ig levels in adults are reduced during the course of ART. 31,29 In this study, patients receiving ART presented a lower expression of IgA in the epithelium, which indicates a recovery of the production of this Ig by the mucosa. On the other hand, it was not observed in the expression of IgG and IgM in the esophageal epithelium. As IgA is the most important effector molecule in the immune system associated with the mucosa, 32 the recovery of the expression of IgG and IgM through ART might have been less effective on the esophageal mucosa surface.
The longer the treatment, the higher the expression of IgA, IgG, and IgM in the esophageal epithelium. These data suggest that after several years of treatment, the alterations in activation and differentiation of T lymphocytes are not totally inhibited by ART. On the other hand, despite the fact that the great part of Igs produced in the course of AIDS is nonspecific, a proportion remains carrying out neutralizing functions. 33 Therefore, higher expression of Igs in the esophageal epithelium could contribute to the defense against microorganisms.
There is strong epidemiologic evidence that the smoking habit has an important role in orogastrointestinal inflammatory and malignant diseases. 34 The development of these diseases is possibly related to the smoking effects on the immune system, including the local immunity of the esophagus. 35
The larger thickness of the esophageal epithelium observed in smoking patients was caused mainly by the increase in the mean diameter of the epithelial cells, since there was no significant difference in the number of epithelial cell layers. Several studies on cellular antioxidant defense mechanisms have shown that the smoking habit increases the oxidative stress in various tissues. 36,37 This condition is associated with cellular lesion, which may lead to the development of hydropic degeneration. One of the characteristics of hydropic degeneration is the increase in the cellular volume caused by a greater entry of water into the cell due to water–electrolyte disturbance. 38
The longer the period of smoking, the smaller the epithelial thickness caused by the progressive decrease in the number of epithelial cell layers. Studies reveal that the cigarette smoke inhibits the alveolar epithelial proliferation and induces apoptosis. 39 On the other hand, the longer the period of smoking, the larger the volume of epithelial cells, which may indicate an aggravation of the oxidative stress in the esophageal epithelium.
Smokers presented a larger number of LCs in the esophageal epithelium than nonsmokers. Similar data were found on the epithelial surface of the lower respiratory tract 40 and on the oral mucosa. These results suggest that either the LCs are able to respond to external toxins or the physical changes in the epithelial barrier induced by toxins demand the presence of a larger number of LCs to preserve the epithelial integrity. 41
However, observing only smoker patients, the longer the period of smoking, the smaller the number of LCs in the epithelium. Possibly, after many years of smoking, the LCs also have cellular lesion due to the cigarette smoke toxins, resulting in apoptosis. 39
Smoking patients presented reduced expression of IgA, IgG, and IgM in the esophageal epithelium. Studies that carried out Ig serum dosages in smokers revealed a reduction in the levels of IgA, IgG, and IgM. 42 The Ig dosages in the saliva and intestinal fluids of smoker patients also indicate a reduction in IgA levels. 43 Smoking might be harming the humoral immunity of the esophageal epithelium.
The longer the period of smoking, the lower the expression of IgG and IgM and higher the expression of IgA in the esophageal epithelium. The IgA is the most important effector molecule in the immune system associated with the mucosa, constituting the first line of immune defense on the mucosal surfaces against pathogenic microorganisms, including viruses. 32 The data collected in this study suggest that after years of smoking, IgG and IgM production is more severely damaged, whereas the IgA expression is increased in an attempt to protect the mucosa against the cigarette toxins.
Candida albicans was identified as the etiological agent in most patients presenting with esophagitis at the time of the autopsy. Candidiasis is the most common cause of esophagitis in patients with AIDS. 44 The C albicans’ ability to colonize, penetrate, and damage host tissues depends on the instability between the fungus virulence and the host’s immune defense. 45 Therefore, immunosuppressed patients frequently present esophageal candidiasis.
Patients with esophagitis presented smaller epithelial thickness caused by smaller mean diameter of the epithelial cells. The epithelial cells are part of the innate immune system, as they are physical barriers important to the defense against pathogens, 13 and studies demonstrate a reduction in the esophageal epithelium in patients with AIDS. 16,17 Probably, these patients had already had thinner esophageal epithelium due to personal characteristics or to a more aggressive HIV virulence, which allowed the passage of microorganisms through the epithelial barrier.
A larger number of LCs was observed in the esophageal epithelium of patients with esophagitis. Immature LCs have a highly active endocytic system with an antigen-processing function. 46,30 After contact with the antigen, they are activated and become mature antigen-presenting cells. 47 Therefore, microorganisms in the esophagus might lead to a larger number of activated LCs in the esophageal epithelium.
Esophagitis led to a higher expression of IgA, IgG, and IgM in the esophageal epithelium. The mucous epithelial nature seems to be an important mechanism for infection and neutralization of infectious agents on these surfaces. The transcytosis of microorganisms along the epithelium may be inhibited by immunoglobulins. 15 Esophageal infections could stimulate the production of IgA, IgG, and IgM in the esophageal mucosa in an attempt to combat the antigens.
The immune status represented by the viral load values and CD4 T lymphocytes count was prejudiced in younger patients. Self-care is not regarded as a male practice, and some authors associate this fact to men’s socialization. 48,49 Moreover, the younger the man, the less he cares about himself. A possible explanation for worse immune status in younger men would be that they would have less adherence to the treatment than the elderly individuals.
Higher values of viral load and lower CD4 T lymphocytes count were also observed in the smoker patients. AIDS develops faster and is more severe in smokers. 50 The smoking habit is associated with a variety of alterations in both humoral and cellular immune systems. Depression of the response to some antigens and a decrease in CD4 T lymphocytes count can be cited among these alterations. 51
The ART reduced the viral load and increased the CD4 T lymphocytes count. These data are in accordance with the literature, which shows that this therapy reduces viral replication, increases the number and improves the function of CD4 T lymphocytes, restores the patient’s defenses, and also increases his chances of survival. 52
Patients with esophagitis presented higher values of viral load and lower CD4 T lymphocytes count. Patients with AIDS frequently have CD4 T lymphocyte counts below 200 cells/mm3, high plasma HIV RNA levels, and clinical manifestations indicating severe immune commitment. In this scenery, opportunistic infections are common. 19
A limitation of this study is related to the small number of cases, since the esophagus was not always present in the general pathology division archives. Another difficulty was the recovery of patients’ clinical data because some clinical records were not found and many of them had incomplete information. However, these limitations become small, given the knowledge acquired in this study.
AIDS causes immune and morphologic alterations in the esophageal epithelium. 16,17 In accordance with the data obtained in this study, age, smoking, use of ART, and development of esophagitis may either reduce or worsen these alterations in the local immunity. It is possible to conclude that the epithelial alterations in patients with AIDS are not caused exclusively by the direct effects of the HIV. The patient’s clinical and behavioral characteristics also have an important role.
Footnotes
Acknowledgments
The authors thank the officials of the General Pathology Division of Triangulo Mineiro Federal University, Uberaba, Minas Gerais, Brazil.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study received grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) and Fundação de Ensino e Pesquisa de Uberaba (FUNEPU).