
Abstract
We present an unusual case of nontyphoidal Salmonella causing an epidural abscess and vertebral osteomyelitis in a severely immunocompromised patient with AIDS as well as a review of the literature. Salmonella vertebral osteomyelitis is exceptionally rare, and this is the first case report in a patient with AIDS.
Introduction
It is well established that Salmonella is an important cause of infection in immunocompromised patients infected with HIV. Salmonella infections can be categorized as typhoidal or nontyphoidal; the latter belongs to a group of food-borne pathogens that cause a spectrum of illness from gastroenteritis to disseminated bacteremia. Often nontyphoidal Salmonella presents as a nonspecific febrile illness and patients are found to have metastatic foci in the bones, joints, central nervous system, and lungs. Although patients with HIV have increased risk of Salmonella infection, there are no reported cases of vertebral osteomyelitis in this population. This case report describes an unusual presentation of nontyphoidal Salmonella causing an epidural abscess and vertebral osteomyelitis in a severely immunocompromised patient with AIDS.
Case Report
A 54-year-old man with AIDS presented with 3 days of rapidly progressing bilateral lower extremity weakness, urinary retention, and fecal incontinence. The patient had difficulty ambulating on the day of admission. The patient denied fevers, chills, nausea, vomiting, diarrhea, headaches, changes in vision, or decreased sensation.
On presentation, the patient’s vitals were remarkable at a temperature of 39.7°C and a pulse of 144 beats per minute. Neurologic examination revealed intact cranial nerves, normal upper extremity examination, 3 out of 5 strength in bilateral lower extremities, and increased tone with hyperreflexic deep tendon reflexes and bilateral Hoffman sign. The patient had no rectal tone and a urinary catheter drained 1.4 L. Initial laboratory results were significant for normal serum electrolytes, creatinine 1.3 mg/dL (baseline 1.0 mg/dL), 12.6 white blood cell s/μL with a normal differential, hemoglobin 9.0 cells/μL, erythrocyte sedimentation rate 119 mm/hr, and repeat CD4 1 cell/μL. Spinal fluid revealed 8 red blood cells/μL, 110 white blood cells/μL with 26% neutrophils, 58% lymphocytes, 16% monocytes, glucose 13 mg/dL, and protein 455 mg/dL. An initial cranial computed tomography (CT) showed mild volume loss and lumbar magnetic resonance imaging (MRI) showed multifocal degenerative disc disease without spinal cord impingement.
Based on the patient’s abnormal spinal fluid profile and neurologic deficits, empiric antibiotics for bacterial and viral meningitis were initiated with vancomycin, ceftriaxone, and acyclovir. Gram stain and culture of spinal fluid were negative for organisms as well as for JC virus, herpes simplex virus, tuberculosis, and cryptococcus. The patient remained febrile at 39.2°C and tachycardic with an unchanged neurologic examination. As meningitis alone did not explain the neurologic deficits, a spinal cord lesion was suspected. The MRI of the cervical and thoracic spine revealed osteomyelitis with discitis at T2/T3, T5/T6, epidural phlegmon communicating circumferentially at various levels from T1 to T8, and dorsal cord compression most pronounced at T4 (Figure 1). A neurosurgical consult determined that drainage was not feasible because of the diffuse infection. On hospital day 4, blood cultures from admission grew Salmonella enterica serovar Typhimurium, and antibiotics were narrowed to levofloxacin for 8 weeks of treatment. Although the patient regained some lower extremity strength, he continued to struggle with ambulation and was discharged to a subacute rehabilitation facility. On a follow-up visit to the infectious disease clinic, the patient was able to ambulate with a walker and was functionally continent.
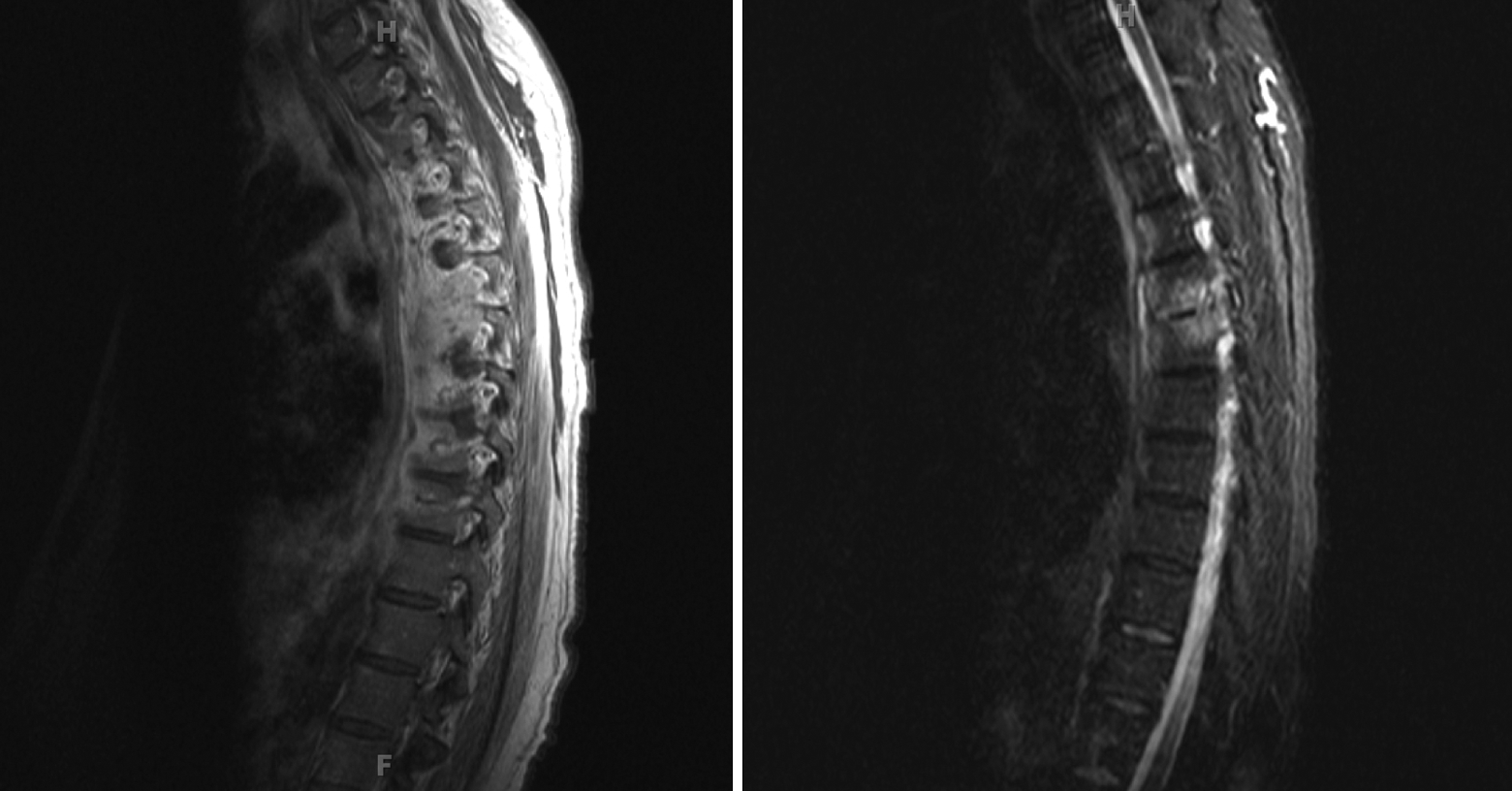
Magnetic resonance imaging (MRI) shows osteomyelitis with discitis at T2/T3, T5/T6, epidural phlegmon communicating circumferentially at various levels from T1 to T8, and dorsal cord compression most pronounced at T4.
Discussion
Vertebral osteomyelitis is a rare condition, with reported incidences between 1:450 000 1 to 2.5:100 000 with a bimodal age distribution. 2 Salmonella vertebral osteomyelitis is even rarer, and only 60 cases have been reported in the English literature. However, this is the first case report of Salmonella vertebral osteomyelitis in a patient with HIV.
Nontyphoidal Salmonella serovars cause 4 clinical syndromes, diarrheal disease, invasive bacteremic illness, focal suppurative infection, and asymptomatic carriage in the stool. In contrast to Salmonella typhi, nontyphoidal Salmonella serovars do not infect the small intestine or gall bladder and primarily cause colitis when gastrointestinal involvement occurs. In immunocompetent individuals, Salmonella infections are often subclinical and almost always self-limited. However, patients infected with HIV frequently present with more severe and invasive infection. This is thought to be due to specific cytokine depletions associated with lower CD4 counts. In immunocompromised hosts, nontyphoidal Salmonella infections are associated with suppurative foci and primary bacteremic disease, which may be recurrent, up to 43%, and more severe on presentation. 3,4
Vertebral osteomyelitis primarily occurs via hematogenous seeding, either from transient bacteremia or from a distant focus of infection, and most commonly infects the lumbar spine. 5 –7 Since clinical imaging almost always reveals disease involving 2 adjacent vertebrae and subsequently their intervertebral disc, an arterial route is the probable source as the segmental arteries supplying the vertebrae bifurcate to supply both adjacent bony segments. In some patients, inflammation of the disc occurs before vertebral infection. 8 In the general population, the most common pathogen is Staphylococcus aureus followed by Escherichia coli. Salmonella is the most commonly implicated organism in sickle cell disease, while Propionibacterium acnes and coagulase negative Staphylococcus are most common in postsurgical infections. In HIV-infected patients with nonvertebral osteomyelitis, the most common bacterial pathogens are Bartonella henselae and Bartonella quintana, but Saureus infections are the most common source specific to vertebral osteomyelitis. 6,9
Although the incidence of spinal infections in patients with HIV is higher than the general population, it is still a relatively rare site of infection even in this population. Therefore, it has been difficult for researchers and reviewers to characterize spinal infections in populations with HIV/AIDS. Weinstein et al reviewed 260 000 patient admissions at the University of Miami/Jackson Memorial Hospital and 7338 of those were HIV-infected patients. In this HIV-positive subset, only 17 (0.23%) had a spinal infection and 5 of those could be linked to intravenous drug use. 9 The study found the incidence of spinal infections in HIV-infected patients to be 23 per 10 000 admissions compared with 7 per 10 000 admissions in the general population. This correlates to smaller studies done at other hospitals. However, none of the infections were due to Salmonella.
Salmonella vertebral osteomyelitis is also rare in the general population and only approximately 60 cases have been reported in the English literature. In the largest review of Salmonella vertebral osteomyelitis, Santos and Sapico summarized the findings of 44 cases. 10 Although HIV was specifically mentioned as a risk factor, no known infections were reported. The incidence of Salmonella vertebral osteomyelitis was greater in men than women, with a ratio of 1.7:1. All infections were monobacterial with S enterica serovar Typhimurium identified as the most common (15%) followed by Salmonella typhi. Fever (87%) and lower back pain (92%) were the most common presenting signs and symptoms. The site of infection was most common in the lumbar spine, followed by thoracic and then cervical spine. Of the reported cases, 48% had positive blood cultures, 41% presented with leukocytosis, 36% of the cases had positive stool cultures, and 23% positive urine cultures. Paravertebral abscesses were present in 39% of the cases while only 4% of cases had epidural abscesses. In total, 72% of the patients were treated with medical management alone and 28% required operative intervention.
Diagnosis, treatment, and follow-up for Salmonella vertebral osteomyelitis are largely the same as vertebral osteomyelitis caused by other pathogens. 10 In a large review, Jensen et al noted that an increased leukocyte count and left shift do not have high sensitivities for the diagnosis of vertebral osteomyelitis. However, increases in the erythrocyte sedimentation rate and C-reactive protein level are highly sensitive and have been reported in up to 98% and 100% of cases, respectively.11,12 Successful treatment depends upon bacterial identification and susceptibility. If blood cultures yield positive results, further invasive testing is not warranted. However, if blood cultures are negative and imaging suggests infection, a biopsy with staining and cultures should be performed. 11 The MRI is the best imaging modality to detect osteomyelitis, epidural abscess, and spinal cord involvement. It is more sensitive than CT or x-ray and is superior in ruling out other diagnoses such as a herniated disk. 6,13 Antibiotics alone are usually sufficient to treat vertebral osteomyelitis. With the exception of infected implanted devices, clinical trials have failed to demonstrate a difference in the efficacy of one pathogen-susceptible antibiotic regimen compared with another. Additionally, intravenous antibiotics have equal efficacy as oral fluoroquinolone therapy. 14 Ideal length of treatment has not been tested by clinical trials; however, observational studies note no significant difference between less than or greater than 6 weeks of antibiotic therapy. 15 Regardless, the recommendations suggest treatment duration of 6 weeks and longer for complicated infections. 16 The CT-guided drainage can be utilized, but open surgery is only indicated if conservative treatment fails or if the patient has infected hardware needing debridement or removal. For the minority of patients with significant vertebral instability, orthopedic back brace, internal fixation, or reconstruction may be required. 6,16 Follow-up at 1 month for signs of clinical improvement is recommended to assess for response to treatment. Further, the C-reactive protein level is more closely correlated with the clinical response to therapy than is the erythrocyte sedimentation rate. 12,17 Repeat MRI is not indicated and one study showed that of all patients who demonstrated clinical improvement, 85% still had MRI findings that were unchanged or worse at 4 to 8 weeks. 18 In another review of 253 patients with vertebral osteomyelitis in Cleveland area hospitals, MRI often performed later in the treatment course did not change the clinical outcomes. 19
In summary, Salmonella can cause invasive infections and may be a marker of advanced underlying impaired immunity, especially in the HIV population. It is critical to identify the causative pathogen in cases of osteomyelitis as targeted therapy is essential to good outcomes.
Footnotes
Acknowledgement
The authors thank Jennifer Dayton Berngard, MD, for her assistance in editing and revising the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.