
Abstract
Nonengagement in HIV care is a major clinical and public health challenge. To identify the risk factors and reasons, we performed (1) a retrospective study of patients admitted to the hospital with advanced HIV disease, (2) a prospective qualitative study, and (3) a population-based area-wide telephone interview. In the retrospective study, clinic care engagement was associated with age (43.9 ± 9.1 years vs 37.9 ± 7.2 years, P = .005) and improved from 23% to 44% (P = .03) after hospitalization. Survival was higher (93% vs 73%, P = .03) among those who engaged in care. Twelve inpatients were interviewed in the qualitative study. Themes identified for nonengagement were social stigma, indifference, or lack of understanding of care needs/denial and life care issues. In the population-based study, 145 patients were interviewed. In all, 49 denied the need for HIV care and 28 denied their HIV status. Stigma, denial, and indifference or lack of understanding of need are significant barriers to care engagement.
Introduction
The population with known diagnosed HIV infection in the United States that is not engaged in care (initially linked and retained) represents approximately 50% of those with known HIV infection. 1,2 Lack of engagement in care has been shown to be associated with increased HIV viral load, a lower CD4 count, 3 and poor survival. 4 Lack of engagement in care dampers proposals that hope to prevent new HIV infections by a test and treat strategy. 1 Studies to date have associated African-American race, drug abuse, lack of motivation, work schedule, depression, and younger age as risk factors for lack of engagement to care. 5 –8
Existing knowledge of the causes of lack of engagement in care has primarily focused on ambulatory populations that include all patients regardless of the disease severity. 5 –8 Less is known about the risk factors for engagement in care in advanced and moderately advanced HIV-infected patients who require hospitalization. 9 The need for hospitalization itself may improve motivation for care but has not been previously studied. Most studies have described risk factor associations for engagement in care, but did not interview patients to probe the rationale behind lack of engagement, especially among those with advanced disease. 10,11 Risk factors for engagement in care at a population-based level are not well known as well as most previous studies were performed among patients who had presented themselves to care in a HIV clinic and therefore have the motivation to seek care. 5 –8 Those who are out of care represent an understudied population. It is likely that those who present to outpatient care may have different motivating factors and greater motivation to seek care than those who sought care only at a time of illness and the need for hospitalization. We proposed first to retrospectively study a group of moderately advanced CD4 <350 cells/mm 3 to advanced patients hospitalized with HIV to determine their risk factors for nonengagement in care and to evaluate whether hospitalization itself, which potentially could convey a need for care, has any effect on care engagement. We then did a prospective qualitative study by conducting interviews to identify reasons for nonengagement in care in a similar population. Finally, we report on a population-based survey among all patients nonengaged in care in a community by identifying those lost to care by the local health department on the basis of lack of laboratory follow-up to determine the risk factors for nonengagement in a population basis. The goal of these studies is to provide insight into the population of patients who are not engaged in care so that targeted interventions could be planned to improve engagement in care with the potential of decreasing HIV-associated morbidity, mortality, and disease transmission.
Methods
Retrospective Study
Starting in July 2007, we performed a retrospective chart study of patients with HIV infection (CD4<350 cells/mm 3 ) who were admitted to a Midwestern, urban (population 1.15 million), US safety net, university-affiliated, 250-bed hospital from 2002 to 2005 with planned clinic follow-up at the same facility. Demographic and clinical variables, including age CD4 count, HIV viral load, antiretroviral drug usage, mental health diagnosis, sex, ethnicity, income source, insurance status, need for transportation services, community resource need acceptance, affect, mood, and coping skills were abstracted from the medical record and from the records of the social services department who saw all the patients. A licensed medical social worker assessed coping as a patient’s ability to deal with and manage their stress; the presence of chronic conditions as the presence of other medical conditions that require frequent medical care; transportation services need as a patient’s perceived ability to get to medical appointments by bus, car, or medically supported transportation; and community resources need acceptance as the assessed need and acceptance of need for case management services including vocational/educational services, financial assistance, housing resources, and food assistance. Engagement in care was defined as keeping 3 or more clinic appointments per year and missing 50% or less of the scheduled visits. Engagement in care 1 year before and after the index hospitalization was calculated. Survival was defined as the patient being alive at the time of chart review (2008-2009) from records of the local health department, hospital records, and the Social Security Administration death index. Bivariate analyses were conducted to determine which variables were significantly related to engagement in care. Independent samples t tests were used for comparisons on continuous variables and chi-square analyses were used for categorical variables.
Prospective Qualitative Study
Using the narrative descriptive method, 12 out-of-care hospitalized individuals with HIV infection and a CD4 <350 cells/mm 3 at the same safety net hospital were identified, and interviews were conducted. Patients admitted between March, 2010 and June, 2011 were approached for participation in the study. Inclusion criteria were (1) age ≥18-year-old hospitalized patients with symptomatic HIV infection and CD4 <350 cells/mm 3 ; (2) not on effective antiretroviral therapy (ART) as evidenced by either not having been prescribed ART or an HIV RNA by polymerase chain reaction >1000 copies/mL; (3) a diagnosis of HIV for at least 1 year, and (4) nonengagement in care, defined as keeping fewer than 3 outpatient clinic appointments or missing more than 50% of the scheduled visits in the previous year (either by self-report or by review of the clinic records). Participants were interviewed by the same researcher during the hospital stay or in the outpatient clinic immediately after hospital discharge. During the hospital admission potential participants were provided a handout explaining the study and written consent was obtained. The interview began by asking “What is it like living with HIV disease?” and then the participant was asked to describe the reasons for not going to clinic appointments and not taking HIV medications. Participants were also asked to describe what could help them to facilitate their clinic visits and to take their HIV medications. The interviews were 30 to 60 minutes in length and at the end of the study written consent was again obtained from the participant to assure that nothing had been disclosed that would be uncomfortable to reveal. Interviews were audio taped, and data were then analyzed. Content analysis was used to examine the data. Three researchers conducted the data analysis, including the physician interviewer, a nurse researcher with in-depth knowledge in qualitative methodology, and a physician researcher with in-depth knowledge of HIV. All 3 researchers read and coded the data independently and then met and agreed on the common themes.
Population-Based Study
Individuals with HIV infection not engaged in care were identified by a local health department between 1998 and 2008 as part of a lost to care project. All laboratories in the metropolitan area report all HIV tests, HIV viral loads, and CD4 counts to the health department. The local health department in Kansas City, Missouri, serves a metropolitan area (7 counties in Missouri) with a population of 1.15 million people. Inclusion criteria for the population-based study included all patients living with HIV infection in the metropolitan area who neither had a CD4 count nor had a HIV viral load testing for 12 months. Nonengaged individuals were identified and contacted by telephone by a health department disease intervention specialist. Individuals who were willing to be interviewed were asked to participate in a telephone interview. Confirmation of lack of engagement of care was done at the time of the phone interview. Participants were asked in an open-ended fashion the reasons why they had not sought medical care, and then specifically asked whether they had difficulty scheduling care, substance abuse, insurance status, transportation issues, financial barriers, or mental health issues. Individual reasons cited by the participants for lack of engagement in care for each encounter were then recorded in a spreadsheet and tabulated.
Ethics
The studies were approved by the University of Missouri-Kansas City institutional review board. Procedures were followed in accordance with the Helsinki Declaration of 1975, as revised in 2000.
Results
Retrospective Study
In the retrospective chart review, a cohort of 64 patients, of whom 1 died during the initial hospital stay, were identified. Among these 63 patients, only 48% (30 of 63) engaged in posthospitalization clinic follow-up, defined as keeping 3 or more clinic appointments per year and missing 50% or less of the scheduled visits. Of the 63 patients, 52 were known to have HIV infection in the year prior to the index hospitalization. Among these 52 individuals, the clinic engagement in care in the year prior to the index hospitalization was 25% (13 of 52), which improved to 45% (23 of 52) in the year after the index hospitalization (P = .031). Only 29% (15 of 52) were on ART prior to hospitalization, which improved to 63% (33 of 52) at the last clinic follow-up. Survival was 73% (24 of 33) among those who did not engage in clinic follow-up and 94% (28 of 30) in those who engaged in posthospitalization clinic follow-up (P = .032). Descriptive, demographic, and clinical characteristics of the group are shown in Tables 1, 2, and 3. Overall, the only variables significantly related to engagement in care were age (P = .005) and acceptance of need for community resources (P = .035). Patients who engaged in care were older and more likely to accept the need for community resources.
Descriptive Comparisons among Those Who Engaged in Care Posthospitalization versus Those Who Did Not Engage in Care.

Abbreviation: SD, standard deviation.
a Statistically significant at P = .05.
Demographic Comparisons of Those Who Engaged in Care versus Those Who Did Not Engage.

Abbreviation: NA, not available.
a Does not meet the minimum requirement of expected values ≥5 in each cell.
Clinical Characteristics of Those Who Engaged in Care versus Those Who Did Not Engage in Care.
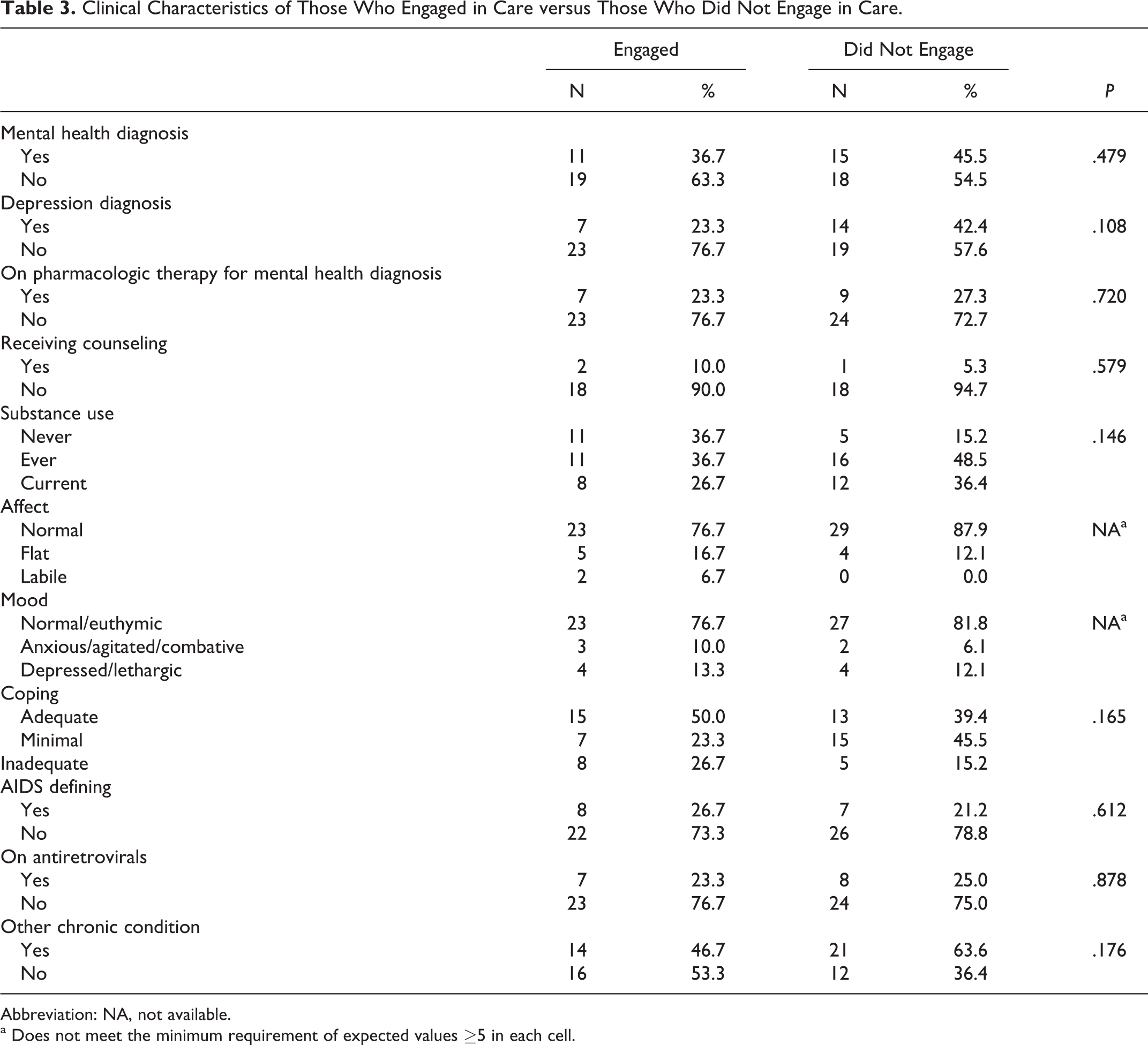
Abbreviation: NA, not available.
a Does not meet the minimum requirement of expected values ≥5 in each cell.
Prospective Qualitative Study
Twelve hospitalized patients with advanced HIV infection who were previously not engaged in care were interviewed individually. There were 6 men and 6 women, 8 African Americans, and 3 Hispanics; their mean age was 44 years and the mean number of years of living with known HIV was 7. Eleven were interviewed during their hospital stay, and 1 during the immediate posthospitalization clinic follow-up. Common themes identified as major barriers to engagement in care were: (1) stigma, (2) indifference/denial and lack of acceptance of HIV, and (3) life issues. Data saturation was reached by the ninth interview and then 3 additional interviews were conducted.
Theme 1: stigma
Participants discussed ways they tried to hide their diagnosis from the ones they loved for fear of being ostracized. Their fear of being “exposed” by taking medications everyday led to a vicious cycle of nonadherence. Participants expressed fear about taking time away from work for clinic appointments to avoid questions regarding the nature of their absence. Alienation among coworkers and rumors at the work place were common, which discouraged some from keeping clinic appointments. Engaging in new employment hampered some in their ability to take time off for clinic visits. Participants were afraid of being alienated at the new work place and did not want to “get fired” because they were taking too much time off from work. One patient described his situation as:
When you first start your job, you are the newcomer so they are going to toss you here and there. So at times I wasn’t able to get done in time to keep my appointments. You know I have finally broke down and I told my mom yesterday. I don’t want to tell my kids because of their attitudes.
Theme 2: indifference, denial, or lack of understanding of need for care and acceptance of HIV status
The chronicity and the insidious nature of the progression of the disease contributed to the lack of adherence to clinic visits. The lack of adequate understanding about the course of the disease accentuated the problem. Participants reported that when they felt fine without any symptoms they did not feel the necessity to keep clinic appointments. As 1 participant said:
I probably would have come… but I felt no symptoms and my body just felt normal. I just couldn’t believe that I have HIV. I wanted to get retested. I don’t know if they were testing it right or wrong. I just started drinking all over and feeling sorry for myself and just gave up. I was intoxicated and drunk.
Theme 3: life issues
Regular clinic visits cut into daily activities. For young men and women with school-aged children, demanding jobs and social commitments contributed to lack of engagement in care. One participant described how she had to deal with her child with special needs and how she rarely thought about herself. She cared more for her daughter than her own health. Arranging for a babysitter each time she had a clinic appointment was very difficult for her. Participants also reported a lack of a relationship with a health care provider as being a factor that contributed to the reason for not keeping their clinic visits. Difficulty accessing the doctor and long wait times in the clinic were also reported as barriers.
Population-Based Study
A total of 381 patients met the inclusion criterion, which represents 9% of those living with HIV in the metropolitan area. In all, 145 were interviewed; 73 refused the interview; and 163 could not be located. Among the 145 patients who gave individual reasons for not seeking care, the reasons for nonadherence quoted by the patients are shown in Table 4. The most common reasons expressed were the denial of need for HIV care and denial of HIV status.
Reasons Provided for Lack of Engagement in Care in a Telephone Survey of 145 Nonengaged People with HIV.

a Included bad experience in a doctor’s office, current incarceration, using nonstandard treatment, mental health, transportation issues, and fear of treatment.
Discussion
In the retrospective chart review, we found that engagement in care improved after hospitalization among individuals with HIV and CD4 <350 cells/mm 3 compared with what was observed prior to hospitalization, but remained less than optimal. We hypothesized that acute hospitalization would give the health care team a chance to communicate with inpatients about the importance of periodic follow-up. During the hospital stay inpatients were visited by a multidisciplinary team consisting of an infectious diseases physician, a caseworker, and an HIV social worker, who provided patient education and linkage to social services. Of the 52 individuals with a prior diagnosis of HIV disease, engagement in care improved from 25% prior to hospitalization to 45% post-hospitalization (P = .031), and those who remained on ART improved from 29% to 63%. Survival was higher (94% vs 73%) in those who adhered to posthospitalization clinic follow-up compared with those that did not (P = .032). Advancing age was associated with an increased clinic follow-up rate, which is consistent with previous reports. 4,7 Those who sought the need for community resources from social services, including housing, establishment of health benefits, and food services engaged in care better than those who did not after the hospitalization (75% vs 41%, P = .035), suggesting that the provision of these services in a vulnerable population can improve care engagement. As an example, 7 of the 8 homeless people engaged in care after hospitalization, during which time the provision of housing services was provided. We were unable to demonstrate an association between mental health disorders, substance abuse users, race, or sex and engagement in care. Similarly, a recent meta-analysis showed retention in care did not differ appreciably between high-risk samples (including drug users and those with mental health disorders) versus more general samples. 13
Attempt to improve engagement in care is dependent on accurately identifying the causes. Few studies have examined the reasons why individuals fail to seek care after a diagnosis of HIV, 14 and fewer yet have sought reasons among those ill enough to be hospitalized. Given the nature of the disease process, the difficult to reach population, and inherent barriers to care, we undertook a qualitative approach to identify specific characteristics and reasons that were potentially contributing to lack of engagement. The common themes revealed in this interview-based approach were social stigma, denial and an indifference to the need for care, and life care issues. Other reasons included lack of adequate patient-doctor relationship and lack of social support. Treisman et al have described that 25% of the patients in the Johns Hopkins AIDS service have the personality type of the stable extrovert, a group that may generate a kind of indifference to HIV risk. 15 This population may be akin to the group which we found that seems to be indifferent to HIV care. Our finding corroborates the importance of the emotional issues that are barriers to adherence, including stigma, fear of side effects of medications, fear of other people knowing, and fear of being seen in a clinic, that has been reported as an abstract by Seekins et al from data collected in a patient survey. 16
To gain an understanding at a community level, we used data from Kansas City Health Department’s lost to care project, which attempted to contact all individuals in the Kansas City, Missouri, area who were lost to care, defined as the failure to obtain a CD4 count in 12 months. This population underestimates those nonengaged in care because the CD4 values may have been obtained in an emergency department visit, or if obtained by an HIV provider it does not necessarily reflect that the result was acted upon in patient follow-up. In a telephone interview, we found that the most common reasons for lack of engagement were not perceiving a need for care and denial of HIV status. A lack of perceived need for care may reflect indifference toward the importance of HIV care. Denial of HIV status may reflect the stigma associated with HIV diagnosis. These findings corroborate the findings found in the qualitative study of hospitalized patients and highlight the importance of the indifference and stigma as barriers to care at a population level.
The limitations of our chart review study include the retrospective nature, single site, and small sample size. Interviews during the qualitative study were challenging because hospitalized patients have frequent interruptions for care, may be receiving sedative medications, and are likely stressed from their underlying illness. The limitations of the phone interview study include that one-third of the individuals who could be located did not wish to participate in the interview, and those that did may have been hesitant in answering questions from the local health department to inquire about their HIV status and care.
Our study showed that the predominant barriers to engagement in care were social stigma, indifference to the importance of HIV care, HIV denial, and a lack of adequate social support. Engagement in care is likely also enhanced by aiding in the provision of social services such as ensuring adequate housing and access to medical care by a provider in whom the patient can form a trusting relationship.
Footnotes
Authors’ Note
This study was presented in part at the Infectious Diseases Society of America 48th Annual Meeting, Vancouver, BC, October 21-24, 2010. The authors thank Breann Smith and Sharon Dean for assistance in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the University of Missouri-Kansas City School of Medicine and the Kansas City Health Department.