
Abstract
Infective manifestations of hematological malignancies can be traced to a variety of pathogens, necessitating broad spectrum empiric antibiotic coverage, and prompt identification of pathogenic microbes to improve clinical outcomes. We present a case of Morganella morganii leading to pneumonia as the presenting illness in a previously undiagnosed, functionally neutropenic adult presenting with acute myeloid leukemia with monocytic differentiation. Our patient was a 64 year old man with no prior medical care who presented with complaints of progressive abdominal pain, productive cough and fevers. Chest radiography revealed no organized consolidations, and computed tomographic imaging of the chest showed bibasilar atelectasis and trace pleural effusions. Laboratory analysis revealed marked leukocytosis with predominant monocytosis, and circulating blasts, suggestive of acute myeloid leukemia with monocytic differentiation, later confirmed with bone marrow biopsy. The patient was initially started on guideline directed empiric therapy for respiratory infection, with sputum cultures later found to be growing Morganella morganii, necessitating a change in antimicrobial therapy, following which the patient showed clinical improvement. To our knowledge, this is the first reported case of Morganella morganii pneumonia presenting at the initial diagnostic encounter of de novo acute myelomonocytic leukemia. This report underscores the need for prompt microbiologic evaluation, broad empiric coverage with early de-escalation, and inclusion of M. morganii in the differential diagnosis of pneumonia in functionally neutropenic patients when standard pathogens are not identified. This case highlights the need to recognize atypical Gram-negative organisms as potential pathogens in these populations, even in the absence of characteristic radiographic findings.
Keywords
Introduction
Morganella morganii is a facultatively anaerobic, rod-shaped, gram-negative bacterium that is ubiquitously present in the environment and colonizes the intestinal tract of both humans and animals. 1 Once considered a low-virulence commensal organism, it has increasingly been recognized as an opportunistic nosocomial pathogen, particularly in association with postoperative wound infections and urinary tract infections. 2 M. morganii is capable of causing a broad spectrum of clinical infections, including but not limited to bacteremia, sepsis, septic arthritis, cellulitis, and necrotizing soft tissue infections. 2
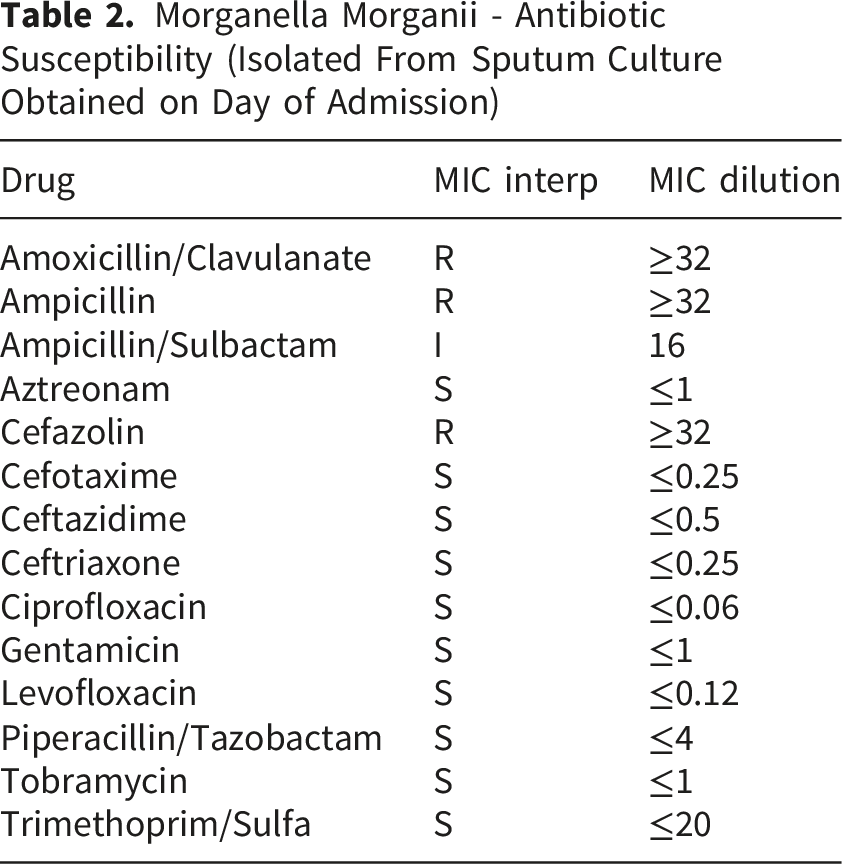
Its evolving virulence, coupled with intrinsic resistance to ampicillin, amoxicillin, and most first- and second-generation cephalosporins—mediated by chromosomal AmpC β-lactamase—poses significant therapeutic challenges.3,4 These resistance mechanisms, along with enhanced pathogenicity, contribute to the increased morbidity and mortality observed in invasive infections.3,4
Respiratory involvement remains exceedingly rare, with only sporadic reports of M. morganii–associated pneumonia, predominantly described in animal models and infrequently documented in humans. 1
Here, we report a case of M. morganii pneumonia presenting as the initial hospital manifestation in a patient with Acute Myelomonocytic Leukemia (AML), highlighting the importance of considering this uncommon pathogen in profoundly immunocompromised individuals.
Case Presentation
Our patient is a 64-year-old male with no significant prior medical history, who presented to the emergency department (ED) with complaints of abdominal pain and dizziness. He reported generalized abdominal pain, predominantly localized to the right upper quadrant, which was gradual in onset and exacerbated by deep inspiration. The pain was unrelated to food intake and resolved spontaneously, only to recur without identifiable aggravating or relieving factors. The patient experienced a marked reduction in oral intake and appetite but denied nausea or vomiting. He indicated that these symptoms began approximately one month prior to presentation but acutely worsened and became continuous over the three days preceding his visit to the ED.
Additionally, he reported dizziness, which commenced approximately one week prior to presentation and was noticeable after exertion or upon standing from a seated position. The patient did not experience loss of consciousness, and the dizziness resolved after a few minutes of rest. Furthermore, he reported feeling feverish and having a cough productive of white sputum for the three days preceding the presentation. The patient denied experiencing any back pain, pain elsewhere, headache, breathlessness, chest pain, dysuria, or contact with sick individuals. He had no history of similar episodes. The patient reported social alcohol consumption and denied tobacco or illicit drug use. He had no significant family medical history and resided at home with his wife and children. There had been no recent changes in dietary habits. He was not taking any medications and had no notable past surgical history, including no recent hospitalizations. The patient was an immigrant who relocated to the United States three years prior to presentation and had not established regular medical care or consulted a physician for many years.
On examination, the patient appeared comfortable at rest, afebrile, and vitally stable, with a saturation of 95% on room air. The physical examination revealed conjunctival pallor. Respiratory examination revealed bilaterally normal vesicular breath sounds with no added sounds. The abdomen was soft, non-tender, with no noted organomegaly, a negative Murphy’s sign, and appreciable bowel sounds.
Laboratory Results From Admission


XR chest PA view from admission. The lack of typical radiographic findings in gram-negative pneumonia may be due to a blunted immune response in the setting of functional neutropenia

CT chest abdomen pelvis with contrast axial STD 2.5, there is bibasilar subsegmental atelectasis. Trace bilateral dependent pleural effusions are also present
Morganella Morganii - Antibiotic Susceptibility (Isolated From Sputum Culture Obtained on Day of Admission)
While the patient was admitted, hydroxyurea, allopurinol, and megesterol were administered to stimulate appetite while diagnostic evaluation was underway. Following the final reports of bone marrow biopsy, the patient elected to seek further therapeutic management at a different tertiary center, as he was eligible for charity care under their provisions.
Discussion
M. morganii is a facultatively anaerobic, rod-shaped, gram-negative enteric bacterium that colonizes the human gastrointestinal tract and rarely causes community-acquired infections. 2 Most infections are nosocomial, occurring after surgery or in hospitalized patients exposed to broad-spectrum antibiotics, and most commonly present as urinary tract and postoperative wound infections. 2 However, its clinical spectrum also includes bacteremia, sepsis, septic arthritis, cellulitis, and necrotizing soft-tissue infections, with rare reports of pneumonia, central nervous system infections, pericarditis, chorioamnionitis, endophthalmitis, and spontaneous bacterial peritonitis. 2
Although M. morganii is globally distributed, it accounts for less than 1% of nosocomial infections worldwide. 5 A population-based surveillance study in British Columbia identified only 62 bloodstream infections caused by the Morganella–Proteus–Providencia (MPP) group over more than a decade. 5 Despite its rarity, the reported mortality rate of 11% highlights the significant clinical impact of this pathogen. 5
In our case, leukemia-associated functional neutropenia likely predisposed the patient to the colonization and aspiration of M. morganii, resulting in pneumonia, a rarely documented infection site for this organism. Although the absolute neutrophil count exceeded 1,500 cells/mm3, only 4% of circulating cells were mature neutrophils, with the remainder consisting of leukemic blasts. This effectively rendered the patient functionally neutropenic, increasing susceptibility to opportunistic Gram-negative infections.
Most reported Gram-negative infections in patients with acute myelomonocytic leukemia occur in nosocomial settings or following chemotherapy. A review of the literature reveals only isolated cases of Morganella infections in patients with hematologic malignancies, including bacteremia in a pediatric patient with acute lymphoblastic leukemia, 6 purulent pericarditis in multiple myeloma, 7 and meningitis in Hodgkin’s lymphoma. 8
To our knowledge, this is the first reported case of M. morganii pneumonia presenting at the initial diagnostic encounter of de novo acute myelomonocytic leukemia.
M. morganii poses significant therapeutic challenges due to its chromosomally encoded AmpC β-lactamase, conferring intrinsic resistance to penicillin, ampicillin, amoxicillin, and most first- and second-generation cephalosporins. 4 Recent genomic analyses have identified emerging carbapenemases, including NDM-1/-5, VIM-1, and OXA-48-like enzymes, along with plasmid-mediated resistance mechanisms, indicating increasing multidrug resistance. Nevertheless, most isolates remained susceptible to third- and fourth-generation cephalosporins, carbapenems, and fluoroquinolones. 4
Prior reports of necrotizing soft tissue infections demonstrated universal resistance to ampicillin and second-generation cephalosporins, with preserved susceptibility to third-generation cephalosporins, carbapenems, and fluoroquinolones. 3 Similarly, a case of neonatal sepsis showed resistance to ampicillin and amoxicillin–clavulanate but susceptibility to ceftazidime, meropenem, gentamicin, ciprofloxacin, and trimethoprim. 9 Accordingly, third-generation cephalosporins, often combined with aminoglycosides, are recommended as a first-line therapy. 9 Carbapenems and fluoroquinolones should be reserved for severe infections or suspected ESBL-producing strains, guided by susceptibility test results.
Despite the inherent limitations of a single-case report and the lack of longitudinal follow-up, this case emphasizes a rare and clinically significant manifestation that expands the known disease spectrum of M. morganii. Prompt empiric antimicrobial therapy, followed by targeted treatment, in conjunction with strict infection control measures, remains fundamental to improving patient outcomes.
Conclusion
Pneumonia due to Morganella morganii is exceedingly rare, and to our knowledge, this is the first reported case in an adult with de novo AMML presenting at the initial diagnostic encounter. This case demonstrates that functionally neutropenic patients may develop serious infections from atypical organisms, even in the absence of classical risk factors like chemotherapy and nosocomial exposure. Given the lack of early radiographic findings in this case, and the emerging resistance profile of M. morganii, prompt microbiological diagnosis and early initiation of broad-spectrum antibiotics are critical. Clinicians should consider M. morganii as a potential respiratory pathogen in newly diagnosed hematologic malignancies when standard pathogens are not identified.
Footnotes
Acknowledgements
We thank the patient and his family for allowing us to share this case to advance medical knowledge.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.