
Abstract
Methicillin-resistant Staphylococcus aureus infection can cause serious illness in children. It can progress to life-threatening bloodstream issues or bone infections, including: deep vein thrombosis, septic pulmonary embolism, toxic shock syndrome, and osteomyelitis. Treatment depends on control of infection with adequate antibiotics and early anticoagulation. We present a case of a 11-year old male child who presented with left arm and right leg pain and swelling that was associated with fever. However, there was no history of trauma. Blood culture was taken and showed Methicillin-resistant Staphylococcus aureus growth. Initial ultrasound of the affected limbs was unremarkable except for subcutaneous edema. On the following day, ultrasound of the affected limbs was consistent with deep vein thrombosis. Additionally, the patient developed pleuritic chest pain and a computed tomography scan with pulmonary angiography demonstrated a filling defect in the left upper segmental artery suggesting septic pulmonary embolism. Magnetic resonance imaging of the lower limbs was recommended and it suggested the diagnosis of osteomyelitis. Ultrasound guided drainage was done and the patient was treated with appropriate antibiotics and enoxaprine. Multifocal thromboembolic events with osteomyelitis in an immunocompetent child are rare and clinically important. This case highlights the complex nature of methicillin-resistant Staphylococcus aureus infection in pediatrics and emphasizes the value of early imaging and multidisciplinary collaboration to establish an accurate diagnosis and a good clinical outcome. Awareness of such presentations can facilitate earlier diagnosis and intervention, to reduce the risk of complications in pediatric patients.
Background
Methicillin-resistant Staphylococcus aureus (MRSA) has emerged as a serious infectious agent worldwide among different age groups generally and pediatric age specifically. Most of these infections are limited to the skin, yet sometimes spread to become life-threatening bacteriemia and bone infections.1,2 The ability of MRSA to cause disease stems from harmful toxins like Panton–Valentine leucocidin (PVL), while resistance to β-lactam antibiotics is attributed to the mecA gene, which alters penicillin-binding proteins, rendering most antibiotics ineffective. 2
MRSA infection can progress to toxic shock syndrome (TSS), septic pulmonary embolism (SPE), deep venous thrombosis (DVT) and osteomyelitis, a testament to the organism’s potential for multisystem disease. TSS is a life-threatening but uncommon manifestation of S. aureus infection, mediated by superantigen toxins that result in overwhelming immune activation presenting as fever, hypotension, and multiorgan failure.3,4
Osteomyelitis is a relatively common infectious disease, whereas venous thromboembolism (VTE) is a rare event in children (1 in 100 000) compared with adults (1 in 1000), but can be very morbid or even mortal.5,6 Pediatric venous thrombosis etiology is more frequently iatrogenic from the usage of central venous catheters. Other risk factors include surgery, trauma, older aged children, congenital pro thrombotic disorders, inflammatory bowel disease, renal comorbidities, short bowel syndrome, infections, and a positive family history of DVTs.5,7,8 The concurrence of DVT and SPE with osteomyelitis is exceptionally rare and diagnostically challenging. Treatment focuses on control of infection with adequate antibiotics, especially against MRSA, and early initiation of anticoagulation.9,10
We present a case of an adolescent male with limping and left arm and right leg swelling who developed a severe disease course of MRSA infection, osteomyelitis, and thromboembolic complications. This case reflects the complex interplay between bacterial virulence, host defense, and thromboinflammatory processes in pediatric sepsis. Clear understanding of these associations is crucial for early diagnosis, proper management, and prevention of disease progression.4,11
Case Presentation
An 11-year-old boy was admitted to the Emergency Department due to left arm and right leg swelling that had persisted for four days. His condition began with pain and swelling around the left elbow, accompanied by a fever of 38.5°C. Plain radiography showed no fractures; thus prompting the application of a supportive splint and sedative management for pain relief. On the next day, the patient developed right leg pain and swelling around the knee joint, along with a transient episode of hallucinations and urinary incontinence, raising concerns about the underlying cause. A blood culture was performed and showed MRSA bacteria growth. The patient had no history of trauma. Past medical and surgical histories are negative and he does not have any known allergies and takes no medications.
During hospitalization, the patient was monitored in the intensive care unit due to abnormal laboratory findings (white blood cell (WBC) count of: 10.6x 10^3/µl, Hemoglobin 12g/dl, C-reactive protein (CRP) 269 mg/L, D-Dimer 16.6, Fibrinogen 767 mg/dL). On physical examination, the patient was alert with a Glasgow Coma Scale (GCS) score of 15/15. However, the left upper limb demonstrated diffuse tenderness and swelling, whereas the right lower limb exhibited swelling extending from just below the knee joint to the toes, accompanied by hotness and tenderness. Additionally, both the left wrist and right ankle had reduced range of motion compared to their contralateral sides.
Furthermore, initial doppler ultrasonography was performed, revealing diffuse subcutaneous edema but no evidence of abscess or fluid collection. As the swelling progressed and pain increased on both limbs, a repeat Doppler ultrasound identified distal DVT in the right cephalic and brachial veins, as well as a filling defect in the right posterior tibial vein below the knee, later on, a subsequent ultrasound showed subperiosteal fluid collection.
Ultrasound-guided drainage of a fluid collection in the right knee was done, and the sample was sent for Gram stain, culture and analysis. Gram stain and culture shows negative results. The synovial fluid analysis showed findings indicating infection, including: turbid reddish fluid with a WBC count of 47,500 (normal range: 0-150), 80% neutrophils, a red blood cell (RBC) count of 800,000, a high pH of 8 (normal: 7.3 - 7.6), low glucose of 1.24 mg/dL (normal: 70-110), and high lactate dehydrogenase (LDH) of 11,934 U/L (normal: 0-240).
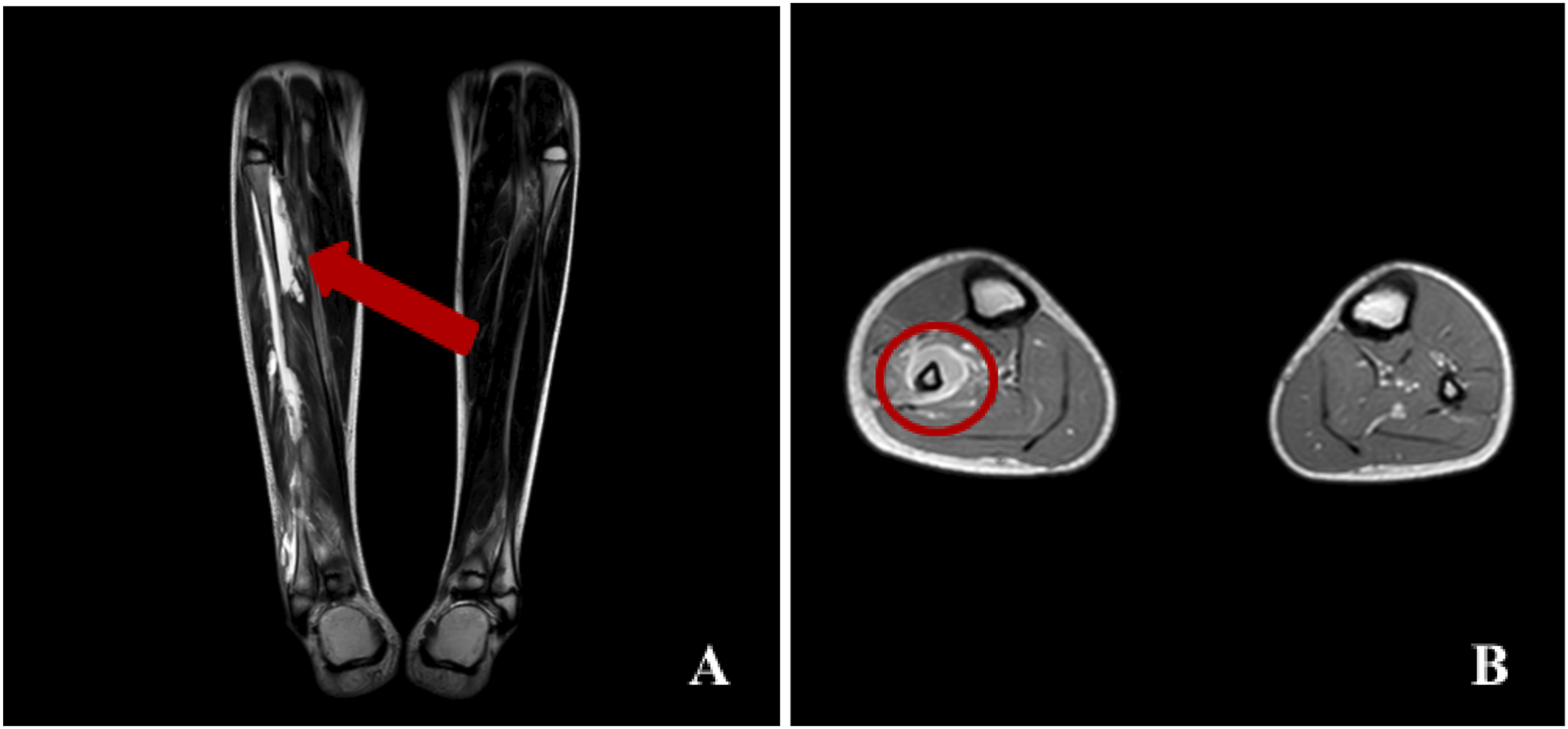
The patient also reported chest pain, raising suspicion for pulmonary embolism. This was confirmed through CT pulmonary angiography Figure 1, which revealed a filling defect in the left upper segmental artery consistent with segmental PE. Multiple bilateral patchy dense consolidation more prominent in lower lobes with minimal left-sided pleural effusion and few prominent axillary, retroperitoneal and hilar lymph nodes were also seen. A follow-up chest CT on the eighth day of admission showed cavitation within a previously noted consolidative opacity in the left upper lung lobe, suggestive of septic emboli. Figure 2. Furthermore, on the seventh day of admission, a second DVT was identified in the right peroneal vein, and magnetic resonance imaging (MRI) suggested osteomyelitis of the right fibula Figure 3. CT with pulmonary angiography demonstrates segmental PE in the left upper segmental artery This sagittal CT image of the chest shows a cavitary lesion with a central air-filled space in the left upper lung zone (A) Coronal MRI of the lower limbs showing increased marrow intensity and cortical destruction in the proximal right fibula; (B) Axial MRI image showing central marrow abscess with surrounding high-signal edema in the right fibula

Although MRSA is a common hospital- and community-acquired organism, the severity and multifocal nature of the infection prompted evaluation for underlying immunodeficiency. The workup revealed no immunologic or malignant abnormalities. The following tests were performed: anti-nuclear antibodies (ANA), rheumatoid factor (RF), HIV, and bone marrow biopsy, showed no underlying malignancy or immunological abnormalities.
Osteomyelitis associated with subperiosteal abscess typically requires surgical irrigation and debridement for adequate source control. In this case, source control was achieved through image-guided drainage of the purulent knee collection in conjunction with targeted antibiotic therapy, without the need for extensive surgical debridement. During the patient’s hospital stay, he started treatment with intravenous (IV) vancomycin 400 mg daily, doxycycline 75 mg IV every 12 hours, and enoxaparin 40 mg subcutaneously every 12 hours. Although the patient initially appeared clinically stable, he developed fever three times within a 24-hour period. This was managed by adding oral ibuprofen 10 ml every 8 hours and switching from vancomycin to intravenous teicoplanin 300 mg every 24 hours.
By the end of the second week, the patient appeared clinically well. He was mostly afebrile, with reduced swelling and improved joint mobility, though mild erythema and warmth persisted in the affected limbs. Laboratory results show improvement: D-dimer 4.7 μg/ml, fibrinogen 669 mg/dL, CRP 78.6 mg/L, WBCs 11.3 x 10^3/µl, and neutrophils 7.9 x 10^3/µl.
Further investigations included echocardiography, which revealed no abnormalities, and abdominal ultrasound, which demonstrated a mildly enlarged liver measuring approximately 14.5 cm in the midclavicular line and an enlarged spleen measuring 12 cm—both larger than expected for the patient’s age. A brain CT scan was unremarkable.
Discussion
The presented case involves a rare and clinically important scenario of an 11-year-old male with a signs of sepsis alongside with multifocal DVT of both upper and lower extremities, pulmonary embolism with radiologic evidence of septic emboli, and osteomyelitis with a subperiosteal abscess. Their coexistence, especially the upper extremity venous thrombosis with the distal lower extremity DVT on the contralateral side, confirmed SPE and adjacent osteomyelitis is an atypical presentation and needs close attention to its pathogenesis, diagnosis and management.
The patient has MRSA infection which can become infectious via wound or invasive procedure. The patient in our case had no injury event. The intense inflammatory response triggered by MRSA leads to the activation of endothelial cells and platelets, resulting in the release of procoagulant cytokines like interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). These mediators upregulate tissue factor expression, enhance fibrin deposition, and reduce natural anticoagulant pathways, so that what occurs in this patient the hypercoagulability state occurs in multiple areas. 12
This case highlights several diagnostic challenges. On the first presentation the patient was managed as a soft tissue infection. The neuropsychiatric symptoms further complicates the clinical picture and shows how early multisystem manifestation of sepsis can distract from the underlying focal source, making reaching a diagnosis challenging for the team. Initial Duplex ultrasound was nondiagnostic and only on repeat imaging shows DVT of cephalic and brachial veins and a peroneal vein filling defect. This highlights that negative early imaging does not exclude developing DVT and serial ultrasound evaluation is often necessary in dynamic infectious processes. MRI showed detailed images which facilitated the understanding of the condition’s complexity. It revealed changes in bone marrow and soft tissue complications, guiding the treatment approach. Finally, the incidental finding of cavitation on chest CT emphasizes the need for chest imaging when bacteremia and limb thrombosis are present, even without prominent respiratory symptoms.
Coordination between pediatrics, infectious disease, orthopedics, radiology, and hematology was essential to optimize antimicrobial therapy, source control, and guide anticoagulation therapy of such a complex case. Empiric Anti-MRSA coverage that was targeted to blood culture positivity (vancomycin and doxycycline). As the patient presented with a fever of 38.5°C and with a positive MRSA blood culture, toxic shock syndrome was considered. While awaiting full susceptibility data, doxycycline was initiated alongside vancomycin because of its preferential tissue penetration and possible inhibitory effects on toxin formation. Antimicrobial therapy was subsequently adjusted according to the clinical course and microbiologic findings. Source control was achieved through MRI-guided recognition of fibular osteomyelitis and subsequently drainage of the purulent knee collection. Despite early initiation of anticoagulation with low molecular weight heparin (enoxaparin) following confirmation of the initial DVT, the patient developed a second distal DVT days later. This progression shows how aggressive and prothrombotic MRSA infection can be, and highlights the need for close follow-up and possible adjustment of anticoagulation during treatment. Anticoagulation therapy was continued in accordance with pediatric thromboembolism guidelines for provoked events, with duration and monitoring tailored to the evolving clinical picture. 13
A published case in the literature described a similar presentation; however, it involved only one limb and did not report any underlying hypercoagulable state. 14 Another comparable case discussed similar complications arising from an infected intravenous catheter, but in an elderly patient rather than a pediatric patient That report emphasized the importance of early catheter removal in minimizing such complications. 15
This report provides valuable insights into the scarce body of literature concerning bacteremia-associated thromboembolic complications in children, especially those with unusual features such as bilateral limb involvement and recurrent SPE. It emphasizes the need for awareness and vigilance in atypical instances of pediatric infection. Additionally, the case highlights the importance of early suspicion and identification of serious complications like DVT and SPE in pediatric bacteremia, which are infrequent and often underrecognized; the shift from localized symptoms to systemic complications was quickly identified and acted upon, potentially reducing morbidity.
The diagnostic approach was comprehensive, involving various imaging modalities (plain radiography, doppler ultrasonography, CT pulmonary angiography, MRI) and laboratory assessments (synovial fluid analysis, bone marrow biopsy), facilitating precise identification of complications including osteomyelitis, subperiosteal abscess, DVT, and SPE. Limitations of this case include unavailable follow up data, due to the patient receiving care across different healthcare facilities, which restricted the assessment of long term outcomes, including: recurrence, post thrombotic syndrome, and growth disturbances.
Conclusion
Multifocal thromboembolic events together with musculoskeletal infection in an otherwise immunocompetent child is rare and clinically significant. It shows the complex and multifactorial nature of MRSA infection in the pediatric population. Presentations of pediatric patients with severe soft tissue or osteomyelitis require maintaining a high index of suspicion for thromboembolic complications, particularly when systemic signs such as fever and respiratory symptoms develop. Appropriate imaging together with collaboration between medical specialties are crucial to reach accurate diagnosis and ensure a favorable clinical outcome. Effective management requires early diagnosis, prompt surgical source control, appropriate anticoagulation and targeted antibiotic therapy.
Footnotes
Ethical Considerations
Our institution does not require ethical approval to report individual cases or case series.
Consent for Publication
Written informed consent was obtained from a legally authorized representatives for anonymized patient information to be published in this article.
Author Contributions
All authors have contributed, read, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset used and analyzed during the current study will be available from the corresponding author upon reasonable request.