
Abstract
I report 2 cases of pleurodesis with 50% dextrose water (DW) in very elderly patients with secondary spontaneous pneumothorax. In both cases, a chest computed tomography scan showed a large pneumothorax with emphysema and multiple bullae. Patients were expected not to tolerate surgical treatment, considering their old age and underlying pulmonary disease. Previously, pleurodesis is performed using other chemical agents. However, chemical pleurodesis can be associated with chest pain, fever, and rarely, respiratory failure. Pleurodesis with 50% DW was performed in 2 patients with resolution of pneumothorax without complications. I recommend that even in elderly patients who could not tolerate surgery or chemical pleurodesis, pleurodesis using 50% DW could be considered because it is relatively safer and effective.
Introduction
Elderly patients with secondary spontaneous pneumothorax are often unable to tolerate surgical treatment. Thus, conservative treatments such as pleurodesis are usually used. When performing pleurodesis with chemical agents such as talc and mistletoe extract (ABNOBA viscum F®), severe complications such as empyema, chronic obstructive pulmonary disease (COPD) exacerbation, and acute pneumonitis could occur. A 50% dextrose water (DW) might be considered a relatively safer agent than other chemical agents, although its mechanism of action remains unknown. Here, I present 2 cases of pleurodesis using 50% DW in very elderly patients with secondary spontaneous pneumothorax, who were improved without any complication.
Case Report
Case 1
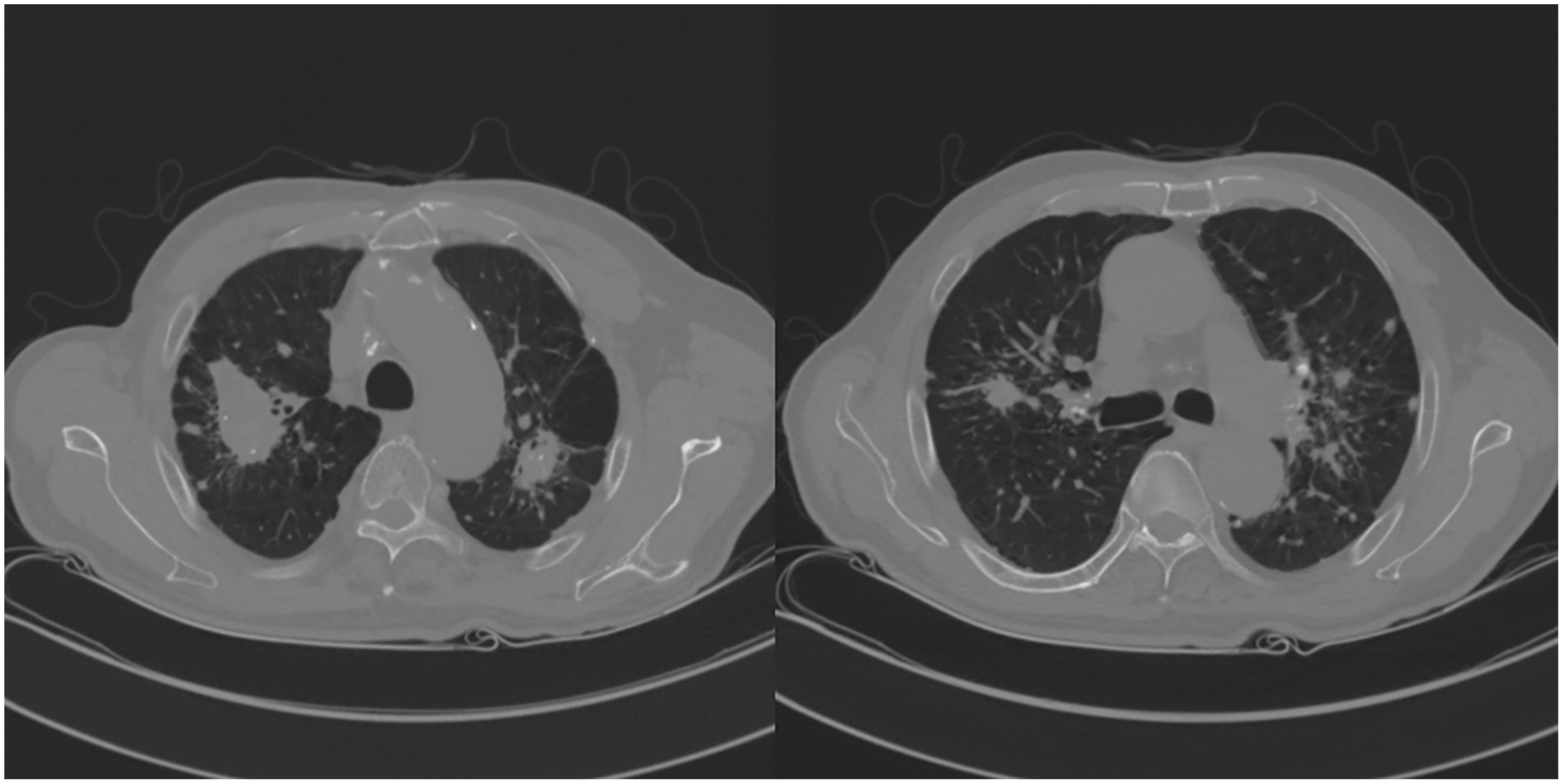
An 88-year-old male presented to our department complaining sudden chest discomfort and dyspnea. Breath sounds on the left side were decreased. The underlying disease was COPD. A large left pneumothorax was diagnosed on chest roentgenography (Figure 1a) and a chest computed tomography scan revealed severe emphysema with multiple large bullae (Figure 2). After closed thoracostomy, massive air leakage had persisted. Given old age and underlying medical conditions, he was expected to be unable to tolerate surgery. Therefore, a pleurodesis was performed using mistletoe extract (ABNOBA viscum F®) on the third hospital day. Symptoms associated with COPD acute exacerbation appeared the day after pleurodesis. He complained of increasingly worsening dyspnea, accompanied by wheezing sound. C-reactive protein levels also rose sharply. Medical treatment was initiated for acute exacerbation of COPD including supplemental oxygen, steroid and antibiotics administration, and nebulizer treatment. After starting the treatment, his symptoms gradually improved. However, massive air leakage persisted. Pleurodesis using 50% DW was performed on the seventh hospital day. The pleurodesis was performed 2 times more at 2-day intervals and the air leakage resolved without complication on the 14th hospital day. The process of pleurodesis was as follows: First, 20 cc of 2% lidocaine was injected through a chest tube for local anesthesia; then, 100 cc of 50% DW solution was injected. The patient’s position was changed to supine, prone, and lateral positions at 30-minute intervals for 2 hours to ensure that the drug was applied to the entire lung surface. To prevent the solution from being immediately drained, the line connecting the chest tube and chest bottle was extended and maintained ~60 cm above the patient. The patient did not complained of any particular discomfort other than mild chest pain. On the 20th hospital day, the patient was discharged in improved condition (Figure 1b).
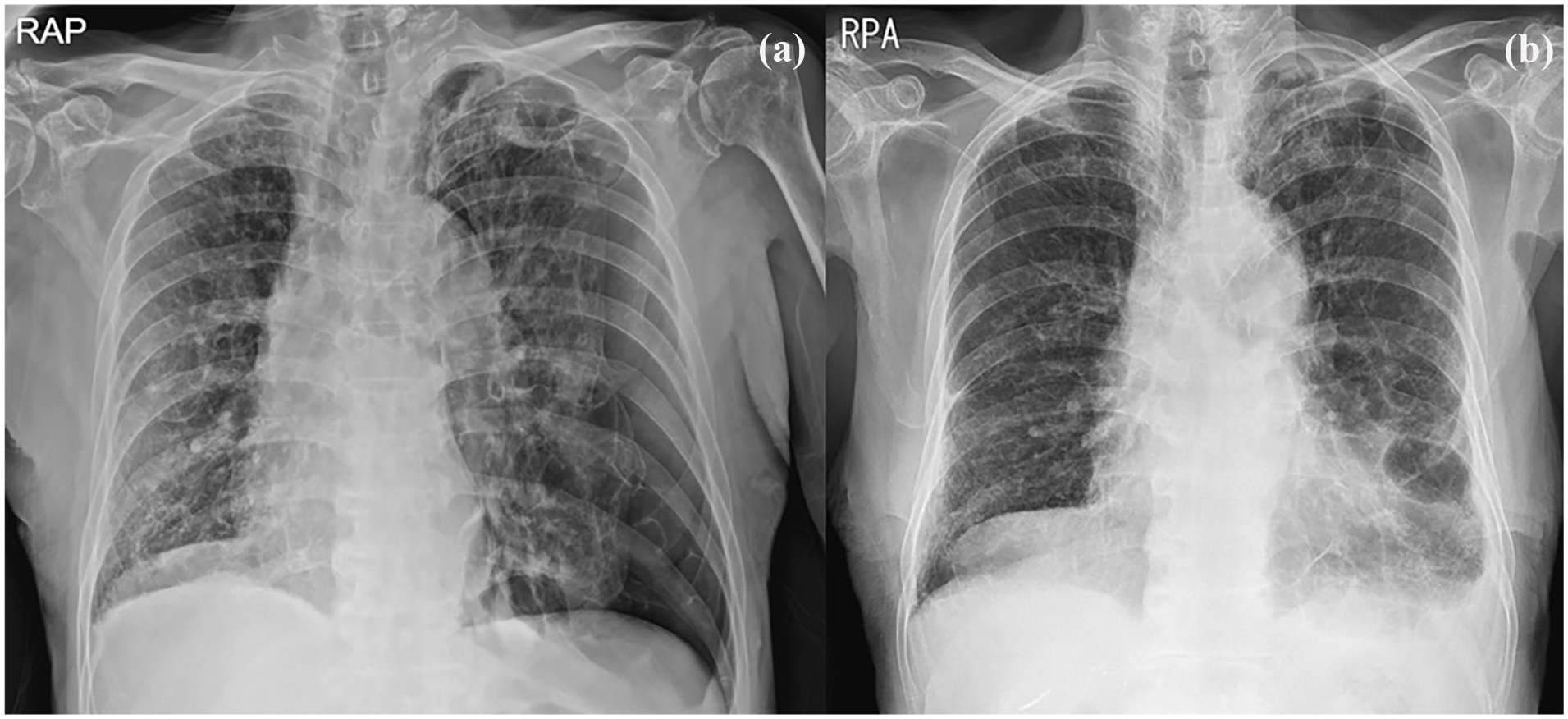
Chest roentgenography (a) showed a large pneumothorax in the left pleural cavity (b) revealed improved state on the 20th hospital day.

Chest CT showed severe bullous emphysema. CT, computed tomography.
Case 2
An 84-year-old male presented to our emergency department with acute dyspnea and chest pain. Breath sounds on the right side were decreased. A large right pneumothorax was diagnosed on chest roentgenography (Figure 3a). The underlying disease was pneumoconiosis with progressive massive fibrosis (Figure 4). A closed thoracostomy was performed, showing massive and persistent air leakage. A month prior, the patient was hospitalized due to right pneumothorax. He underwent pleurodesis using talc slurry considering his old age and medical condition. As the patient was expected to have a very high risk of recurrence in the future, we decided to perform pleurodesis using 50% DW on the first hospital day. Pleurodesis using 50% DW was performed twice with resolution of the air leakage without complication on fifth hospital day. Pleurodesis was performed in the same process as described above at 2-day intervals. The patient did not complained of any particular discomfort. On the sixth hospital day, the patient was discharged (Figure 3b). It has been 3 months since his discharge. There has been no sign of recurrence.

Chest roentgenography (a) showed a large pneumothorax in the right pleural cavity (b) revealed improved state on the sixth hospital day.
Chest CT showed pneumoconiosis with progressive massive fibrosis. CT, computed tomography.
Discussion
The most effective treatment for spontaneous pneumothorax is surgery. For patients who cannot tolerate surgery, pleurodesis might be the second choice of treatment. Conventional chemical pleurodesis agents include erythromycin, tetracycline, and talc slurry.1,2 When performing pleurodesis using these agents, complications such as pleuritic pain, empyema, COPD exacerbation, and acute pneumonitis could occur. In very elderly patients, complications could have fatal consequences. In addition, effects of pleurodesis are sometimes equivocal. Although the mechanism of action of 50% DW is not clearly known, it might be a relatively safer agent compared to other chemical agents.3 -5 In this report, patients were improved and discharged without any complications after undergoing pleurodesis using 50% DW. There has been no evidence of recurrence for several months.
Conclusion
In very elderly patients with secondary spontaneous pneumothorax who have severe underlying lung diseases and high surgical risk, pleurodesis using 50% DW could be a safe and efficient option.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.