
Abstract
Inflammation is a major pathogenic pathway in pulmonary chronic obstructive disease (COPD). Interleukin-6 (IL-6) mediates the local and systemic immune response. The aim consisted in investigating the relationship between IL-6 serum levels and IL-6 -597A/G gene polymorphism (rs1800797) with COPD. Serum levels of IL-6 were determined using an enzyme-linked immune-sorbent assay, in 120 participants (60 COPD patients and 60 healthy subjects), from Transylvanian region. The IL-6 -597A/G gene polymorphism was investigated by high molecular weight genomic DNA extracted from the peripheral blood leukocytes, and subsequently analyzed by the Polymerase Chain Reaction Restriction Fragment Length Polymorphism (PCR-RFLP) technique. Smoking history, the severity of the disease, expressed by the GOLD stages, and arterial blood partial pressure of oxygen (PaO2) levels were also investigated. COPD patients had significantly elevated blood levels of IL-6 when compared to the control group (p < 0.05). The frequencies of AA, AG, and GG genotypes were 61.6%, 26.6%, and 11.6% in the COPD cases and 70%, 23.3%, and 6.7% in healthy subjects, respectively. There were no statistically significant differences in IL-6 rs1800797 genotypes and allele frequencies between cases and controls (χ2 = 0.54, OR = 1.29 and χ2 = 0.21, OR = 1.48, respectively). Higher serum levels of IL-6 were found in the GG genotype subgroup in COPD patients. IL 6 levels are higher in COPD patients, where positively correlate with pack-year index, but not with clinical features. Although COPD patients did not have statistically different rs1800797 allele distribution compared to healthy subjects, the GG genotype is associated with higher IL6 serum levels.
Introduction
Chronic obstructive pulmonary disease (COPD) represents a major health problem worldwide, with more than 3.0 million deaths in 2016, according to a 2018 Report of World Health Organization (WHO). 1 The disease is defined by persistent and progressive respiratory symptoms (dyspnea being the most debilitating one), airflow limitation (which is not fully reversible), and inflammatory response, local or systemic, 2 often correlated with other extrapulmonary effects. 3 Smoking is responsible for the occurrence of various pathologies, acting as a major risk factor of COPD, determining local and systemic inflammation.4–7
Inflammatory biomarkers represent a subject of constant research interest. Interleukin 6 (IL-6) is a four helical protein of 184 amino-acids, produced, mainly, by T Lymphocytes and macrophages, with the corresponding gene located on chromosome 7p21. 8 It represents one of the various pro-inflammatory cytokines involved in the pathogenesis of COPD, 9 but it also acts as an anti-inflammatory molecule. 10 IL-6 regulates local and general immune and inflammatory responses, by representing a major factor in the maturation of B and T lymphocytes. 11 Systemic persistent inflammation in COPD patients, as revealed by measuring markers such as IL-6, C Reactive Protein (CRP), TNF-α, 12 seems to be related to accelerated lung function decline and associated with acute exacerbations of COPD. 13 Numerous studies have tried to determine if IL-6 serum levels are associated with COPD 14 or it’s severity, 15 clinical outcome, 12 or mortality. 16 The various limitations of these studies and conflicting results, however, represent the reason why the involvement of IL-6 in COPD pathogenesis remains controversial.
Genetic testing has a major contribution to the development and progression of diseases and disorders, 17 including emphysema 18 and COPD. 19 In the past decade, research was focused on the genetic risk factors, with interesting results regarding Single Nucleotide Polymorphisms (SNPs). SNPs are defined as the most frequent form of genetic variation in the human genome, occurring when a single nucleotide is replaced with another one in a certain stretch of DNA. SNPs can be used to determine the response to environmental factors, 20 the susceptibility for certain diseases, 21 or the response to drug therapy. 22 The most frequently investigated IL-6 SNP is rs1800795 (or -174 G/C ) which was associated with cardiovascular diseases, 23 psoriasis, 24 breast cancer, 25 and higher inflammatory markers levels. 26 No association was found between rs1800795 and lung cancer. 27 IL-6 -597G/A (rs1800797) and -572G/C (rs1800796) were also studied in relation with various diseases. 28 Several studies have been conducted regarding IL-6 gene polymorphisms and the risk of COPD, but with controversial results. One study showed a protective role of IL-6 -572G/C polymorphism and no association of IL-6 -597G/A and IL-6 -174G/C polymorphisms with COPD, 29 while others revealed that IL-6 -174G/C SNP is associated with lung function decline and susceptibility to COPD in smokers. 30 Nevertheless, few information regarding rs1800797 polymorphism are found in the literature. The G allele is considered the normal wild type, while the A allele was identified as minor in several populations worldwide, but not in Romanian or east-European ones, with varying minor allele frequency (MAF; 0 in Vietnamese population, 0.13 worldwide to 0.495 in northern European or Baltic populations). 31
The study aimed to determine if IL-6 serum levels are correlated with clinical features of COPD and also to investigate the rs1800797 polymorphism in the Romanian population and it’s relation with COPD.
Materials and methods
Study overview
General
A case–control study 1:1, including 120 participants (60 COPD patients and 60 healthy controls), approved by the Local Research Ethics Committee of “Iuliu Hatieganu” University of Medicine and Pharmacy Cluj-Napoca (No. 298/29.06.2016), was conducted in the North-Western part of Romania, between July 2016 and December 2019. Written informed consent had been obtained from all the participants. COPD diagnosis and classification of stages was based on 2017 Global Initiative for Obstructive Lung Disease (GOLD) guideline. 2
Exclusion criteria
Age under 40 years or over 90 years, previous diagnosis of other chronic lung diseases (asthma, interstitial lung disease, and obstructive sleep apnea syndrome) or any acute pulmonary disease, chronic or acute heart disease (congestive heart failure, acute coronary syndrome, recent revascularization, and oral anticoagulant therapy), recent thoracic surgery, kidney failure, neoplasia (active or history of), autoimmune diseases, allergies or genetic disorders, and treatment with oral corticosteroids.
Anamnestic data
Smoking status was evaluated by the history of exposure and pack-year index. Patients were divided into active smokers (AS), non-smokers (NS), and former smokers (FS). A 65 years old cutoff limit was considered, as rs1800797 was found to be involved in different pathologies in this population subgroup, regardless of gender.32,33
Functional respiratory tests
Spirometry was performed according to the American Thoracic Society and European Respiratory Society guidelines, 34 using a Master Screen Care Fusion Jaeger Spirometer. COPD diagnosis required value of the Tiffneau Index lower than 0.7. 35 Forced Expiratory Volume in the first second (FEV1s), FVC (Forced Vital Capacity), Tiffneau Index, and MEF50 (Maximal Expiratory Flow at 50% of Vital Flow Capacity) were determined and expressed in percent of the predicted value after inhalation of 400 μg Salbutamol, to appreciate the severity of the FEV1s decline.
Peripheral blood measurements
Venous blood samples (5 ml) were collected in vacutainer tubes without anticoagulants from cases and controls on their first day of admission. The blood was centrifuged for 15 min at 4000 rpm at room temperature (20°C–25°C). The serum was collected and then stored at −80°C until enzyme-linked immune-sorbent assay (ELISA) assay was performed. The arterial blood oxygen partial pressure (PaO2) was determined by radial artery puncture, in sitting position, breathing room air, early in the morning.
Determination of IL-6 levels by ELISA technique
An Enzyme-Linked Immunosorbent Assay kit (Boster Picokine™ Human IL-6 Pre-Coated ELISA) (Boster Biological Technology, 3942 Valley Ave, Pleasanton, CA, USA) was used. The sensitivity of the minimum detectable dose was 0.3 pg/ml, with a detection range between 4.69 and 300 pg/ml. The samples were defrosted overnight at 4°C, and in the day of procedure, all reagents and samples were kept at room temperature for 1 h. And the reading was performed at 450 nm wavelength. After obtaining the standard curve, the results were extrapolated for the absolute concentrations using the Magellan3 program. The measurements were carried out in duplicate as a batch test.
Genotyping conditions
Peripheral blood samples were collected from all participants in Ethylenediaminotetraacestic acid (EDTA)-coated tubes using standard antecubital venepuncture method, after overnight fasting. DNA samples were obtained from 300 μl blood, using Wizard Genomic DNA Purification Commercial Kit (Promega Corporation, Fitchburg, WI, USA). Genotyping was based on Polymerase Chain Reaction Restriction Fragment Length Polymorphism (PCR RFLP) technique. The investigated polymorphism was: rs1800797 (IL-6 -597A/G). The amplification products were submitted to enzyme digestion with 4 units of FokI (Fermentas; Thermo Fisher Scientific, Waltham, MA, USA) and analyzed by electrophoresis agarose gel (MetaPhor®; FMC BioProducts, Rockland, ME, USA), allowing detection by ethidium bromide staining of the corresponding genotypes: AA (527 bp), GA (527 and 461 bps), and GG (461 bp).
Statistical analysis
The statistical analyses were performed using IBM Statistical Package Program for the Social Sciences version 20 and GraphPad 5 software. Data were expressed as mean ± standard deviation (SD), absolute and relative frequencies. The significant difference between groups and demographics was determined by the Student’s t-test and ANOVA test. To analyze the frequencies of the IL-6 genotypes and allele in cases and controls, Pearson’s chi-square and Fisher’s exact tests were used. In order to estimate the sample size for our study, we searched the available literature data and identified the presence of variants in different ethnic groups, using ClinVar program. We also investigated the presence of variants in population and applied the goodness-of-fit test to evaluate the Hardy-Weinberg equilibrium for the distribution of the genotypes of the patients and the controls. The assessment of risk factors was performed by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from binary logistic regression analysis, and Fisher’s exact tests. A p-value lower than 0.05 was regarded as statistically significant. For the statistical analysis of IL-6 serum levels, GraphPad Prism 5 software was used, with unpaired t-test with Welch’s correction and a p ⩽ 0.01 setting.
Results
Demographic and paraclinical characteristics
The demographic characteristics of the participants were similar according to the mean age, the predominance of males, and smoking status (Table 1). There is a statistically significant difference between the COPD group and the control group, in terms of functional respiratory tests (FEV1s, FVC, Tiffneau Index, MEF50).
Demographic characteristics and clinical outcome of the study and control group.

n: number of individuals; SD: standard deviation; NS: nonsmokers; AS: active smokers; FS: former smokers; BMI: body mass index; FEV1s: forced expiratory volume in the first second; FVC: forced vital capacity; MEF50: maximal expiratory flow at 50% of vital flow capacity; PV: predicted value; COPD: chronic obstructive pulmonary disease; PaO2: partial pressure of oxygen
Values are expressed as mean ± SD.
Based on the Student’s t-test.
Based on chi-square test.
The goodness to fit test was performed, revealing the presence of Hardy-Weinberg equilibrium in genotype frequencies both for healthy subjects (chi-square test p = 0.056) and for COPD patients (chi-square test p = 0.028), with a p cut-off value of 0.05.
Allele and genotype frequencies
G allele was found to be the minor allele, with a presence of 25% in COPD and 18.33% in healthy subjects (Table 2). When assessing the relationship between genotype and COPD, no statistical significance was observed for AA versus AG genotype (p = 0.54, OR = 1.297, 95% CI = 0.55–3.01), for AA versus GG genotype (p = 0.29, OR = 1.98, 95% CI = 0.53–7.32), or for AG versus GG genotype (p = 0.55, OR = 1.53, 95% CI = 0.36–6.35). Also, no statistical significance was revealed when studying the dominant effect of the G minor allele (p = 0.21, OR = 1.48, 95% CI = 0.79–2.76).
Distribution of genotypes and allele in COPD group and control group.

n: number of patients; COPD: chronic obstructive pulmonary disease
Correlations between IL-6 serum level and characteristics of patients
The serum concentrations of IL-6 in COPD patients compared to controls were significantly higher (5.06 pg/ml ± 1.75 vs 3.81 pg/ml ± 0.4; p < 0.001; Figure 1), although the serum levels of IL-6 did not correlate with the severity of the disease (p = 0.16, r = 0.18), or PaO2 level (p = 0.62, r = 0.06; COPD patients had a mean ± SD of PaO2 level of 71.9 ± 19.4 mmHg). When smoking history of pack-year index was considered, a positive correlation with IL-6 levels (p = 0.031, r = 0.19) was found, but not with smoking abstinence time in years (p = 0.63, r = 0.04).

IL-6 serum levels detected by ELISA method in COPD patients versus controls.
No difference was observed when analyzing the decline of FEV1s and FVC related to different alleles in IL-6 rs1800797 (Table 3).
FEV1s and FVC values for different alleles in IL-6 rs1800797 in COPD patients.

FEV1s: forced expiratory volume in first second; FVC: forced vital capacity; p value: Student’s t-test; CI: confidence interval
The IL-6 serum levels were statistically significant higher in COPD patients for AA (4.9 ± 1.28 vs 3.81 ± 0.43, p < 0.01) and GG (6.41 ± 1.66 vs 3.69 ± 0.1, p = 0.011) but not for AG (4.84 ± 2.47 vs 3.83 ± 0.38, p = 0.14; Figure 2).
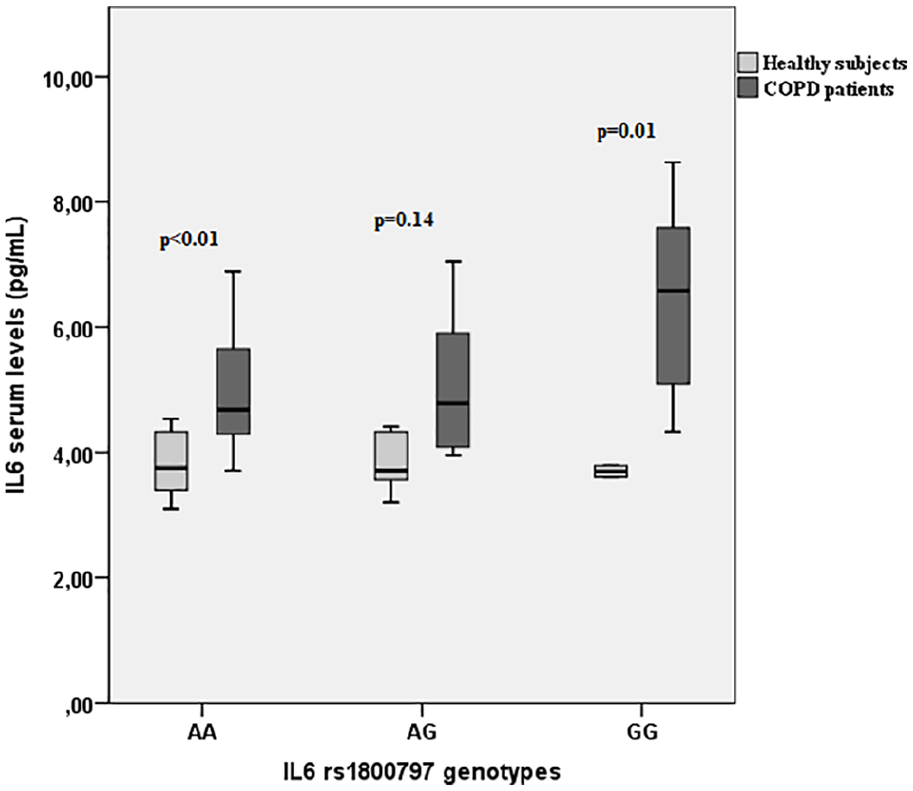
IL-6 serum levels according to AA, AG, GG genotypes in COPD patients and healthy subjects.
In COPD patients, the highest levels of IL-6 were found in the GG genotype but without statistically significance (p = 0.096, ANOVA test), while in healthy subjects the values were similar among groups (p = 0.831).
Distribution of allele and genotype among groups
The distribution of the G minor allele and the homozygous GG variant genotype according to sex, age (when a limit of 65 years old cutoff limit was considered), smoking status (smokers vs nonsmokers), the severity of COPD (mild vs moderate + severe COPD), and PaO2 level, revealed no significant differences (Table 4).
Distribution of minor allele G and homozygous GG variant genotype of IL-6 -597A/G gene polymorphism according to sex, age, smoking status, severity of COPD, and PaO2 level.
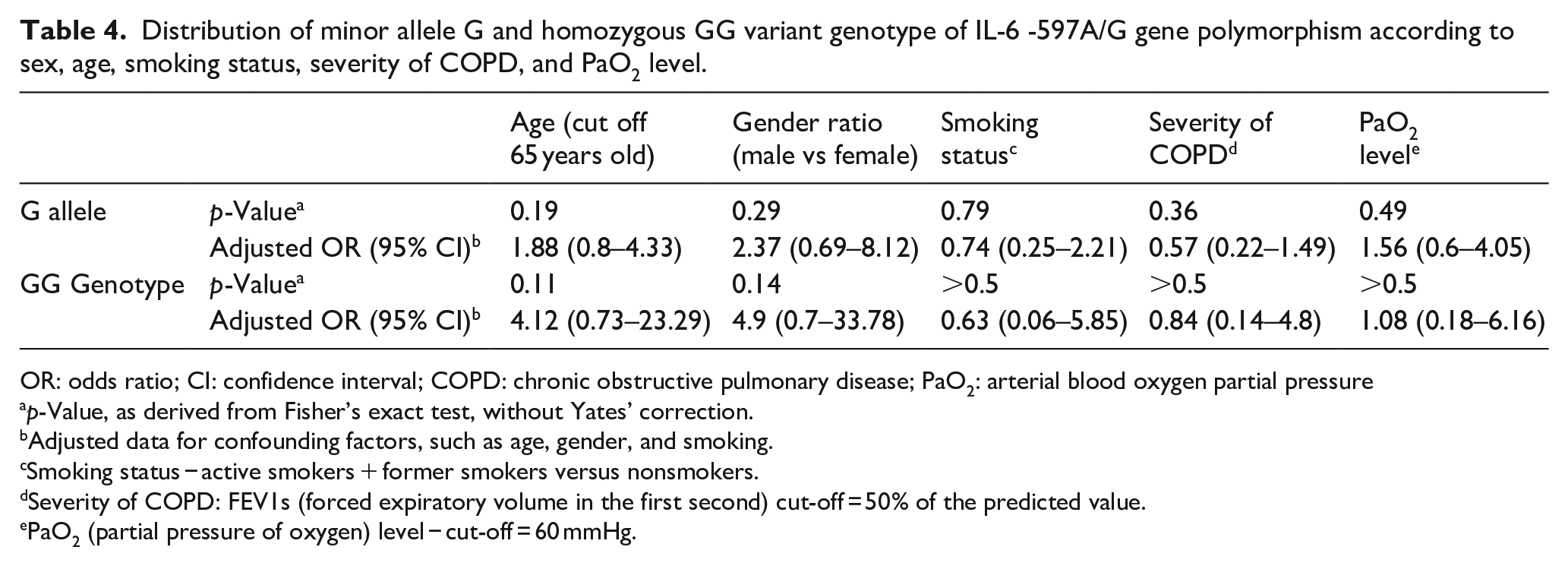
OR: odds ratio; CI: confidence interval; COPD: chronic obstructive pulmonary disease; PaO2: arterial blood oxygen partial pressure
p-Value, as derived from Fisher’s exact test, without Yates’ correction.
Adjusted data for confounding factors, such as age, gender, and smoking.
Smoking status − active smokers + former smokers versus nonsmokers.
Severity of COPD: FEV1s (forced expiratory volume in the first second) cut-off = 50% of the predicted value.
PaO2 (partial pressure of oxygen) level − cut-off = 60 mmHg.
Discussion
The exact pathogenesis of COPD is not completely elucidated. Both local and systemic inflammation in COPD could be explained by the innate immunity (through neutrophils, macrophages or eosinophils) and also adaptive immunity (through T and B Lymphocyte cells), 36 but the involvement of epithelial and endothelial cells or fibroblasts plays an important role as well. 37 Recent studies found that cigarette smoking is a major environmental trigger and the most incriminated risk factor of COPD, which is rather a multifactorial disease, as only 20% of smokers may develop COPD. 36 Biomarkers of tobacco exposure, like carbon monoxide concentration in exhaled air, represent useful tools in assessing smoking habits. 38 Strong evidence suggests that inflammatory processes in COPD can be found in the airways, lung parenchyma, and pulmonary vascularization but also the systemic circulatory system.37,39
In our COPD group, 80% of the patients are active smokers or ex-smokers, a higher percentage than in controls or in the general population. The results are similar to the ones in the Rotterdam study, where higher COPD prevalence was found in smokers. 40 Liu et al. conducted a study on 4135 smokers aged ⩾45 years and found that 58.3% of those who had smoked for more than 30 years continued smoking habits compared with 7.5% of those who had smoked up to 9 years. 41 Our study revealed a positive correlation between IL-6 and pack-year index, indicating that cigarette smoking could be a major contributor to systemic inflammation in COPD patients. No correlation of IL-6 levels was found with years of smoking abstinence, similar to other studies. Reichert et al. also found no statistically significant differences in the decline of serum levels of IL-6 and CRP during a smoking cessation program. 42
IL-6 is a pleiotropic pro-inflammatory and immunomodulatory cytokine that also acts as an antiinflammatory myokine. 8 Our study revealed higher serum levels of IL-6 in the COPD group versus healthy subjects, suggesting the implication of systemic inflammation in COPD patients. These results are consistent with literature data. Wei et al. reported, in 2015, that serum IL-6 concentrations are higher in stable COPD patients than in healthy controls, indicating that IL-6 serum level might serve as a useful tool in investigating early pulmonary function changes in COPD patients. 43 The plasma IL-6 levels are associated with high CRP levels via hepatic production,44,45 but the mean serum level of IL-6 is a more sensitive biomarker to predict inflammation. 46
Previous studies focused on identifying a possible association of IL-6 plasma concentrations and the severity of the disease, to define the role of IL-6 in COPD pathogenesis. De Moraes et al. reported no association of IL-6 serum levels with the severity of COPD in ex-smokers, 47 in contradiction with other studies that proposed a novel phenotype of COPD patient, characterized by a strong association between poor clinical outcome and persistent systemic inflammation (demonstrated by elevated IL-6 levels). 12 Our study found no association between serum IL-6 levels and severity of COPD (FEV1s, PaO2 level), but a positive correlation was found between IL-6 serum levels and smoking history, quantified by the pack-year index.
Hashimoto et al. conducted an experimental research on animal models and found that the administration of antibodies against IL-6 receptors reduces chronic hypoxia through underlying mechanisms currently insufficient explained, but with an important contribution to new therapeutic directions for COPD patients with signs of pulmonary hypertension. 48
The COPD patients included in this research had no chronic heart failure, acute coronary syndrome, or overlapping obstructive sleep apnea as other causes responsible for systemic inflammation. 49 About 30% of our COPD patients had lower PaO2 levels (less than 60 mmHg), and 68.3% of them had moderate to severe COPD. Hypoxemia, as a result of alveolar hypoxia, represents a major cause for disability in COPD patients, and it is associated with increased systemic inflammation. Nevertheless, no association between the PaO2 level and IL-6 serum levels was found in our research.
Genome-wide association studies represent an actual concern in terms of identifying new loci and potential targeted therapies. 50 Numerous SNPs in alpha 1-antitrypsin, tumor necrosis factor, microsomal epoxide hydrolase, glutathione S-transferase, interleukin-6, interleukin-8 genes have been studied in terms of association with COPD susceptibility, severity, phenotypes, drug response, or comorbidities, but with conflicting results and limitations of the studies.51,52 In 2009, two case–control studies comprising 1488 participants, conducted by He et al. 30 revealed that out of seven IL-6 SNPs, four were associated with COPD, while the rs1800797 allele was associated with a rapid decline in lung function. Another European study investigated the relationship between rs1800797, rs1800795, and rs1800796 and the susceptibility for the disease, the lung function, and hypoxemia level and concluded that rs1800797 and rs1800795 were not associated with the disease, the frequency of genotypes containing the C allele was lower in COPD patients, and also that the GCG (-597, -174, -572) haplotype was associated with the disease. 29 In a Chinese Han population, a case–control study revealed 7 SNPs associated with COPD, rs1800797 not being one of them. 53 In 2016, Dou et al. found no significant association between rs1800797 and COPD. 54 In our study, the minor allele was found to be the G allele (25% of COPD patients and 18.33% in healthy subjects) but was not associated with the severity of the disease, smoking status, or PaO2 level. The variant genotypes, AG and GG were present in 38.33% of COPD patients, and no association with the disease was found. Our results are consistent with previous studies that showed that the decline of FEV1s and the susceptibility to COPD in smokers is not associated with rs1800797 gene polymorphism. 29 In 2016, Lorente et al. found that the rs1800797 polymorphism is associated with lower IL-6 serum levels and better survival rates. 55
Also, we analyzed the correlation between genotypes and the serum levels of IL-6. When considering the genotypes, the GG group had higher serum levels of IL-6 in COPD patients, with borderline 56 significance (p = 0.096). This indicates that rs1800797 could be involved in the development of systemic inflammation.
We studied the importance of IL-6 levels and IL-6 -597A/G polymorphism in the development of COPD, the severity of the disease, smoking status, and PaO2 level in COPD patients without major comorbidities. SNPs are known to show important inter-ethnical differences. To our knowledge, this is the first study of the IL-6 SNP in a Romanian cohort of COPD patients, and the first one to evaluate the distribution of allele and genotype frequencies of rs1800797 according to demographic, clinical outcome characteristics, and IL-6 serum levels.
Identifying risk factors that contribute to the pathogenesis of COPD could serve as a useful tool in selecting high-risk group populations and earlier implementation of specific therapeutic strategies. More large-sized and prospective studies are necessary to evaluate the relationships between gene polymorphisms and COPD susceptibility, phenotype, lung function, and drug effects, in different ethnic groups.
Study limitations
The small sample of subjects included in this study (60 COPD patients and 60 healthy subjects) is explained by the numerous exclusion criteria (initially, 485 patients were included in the study), to exclude any pathology that might lead to increased levels of circulating IL-6, independent of COPD. Another limitation of the study consisted of the exclusive Romanian provenience of cases and controls and rather moderate to severe stages of COPD.
Conclusion
IL-6 serum levels are higher in COPD patients, where positively correlate with pack-year index, but not with FEV1s or PaO2 level. IL-6 serum levels are higher in COPD patients with the GG genotype of IL-6 rs1800797 polymorphism. There is no association between GG genotype or G allele and COPD. FEV1s and PaO2 in moderate and severe COPD patients are not influenced by the presence of the minor G allele G or the homozygous GG variant genotype of IL-6 rs1800797 polymorphism.
Footnotes
Author contributions
A.F.C.: concept, methodology, investigation, data collecting, writing, editing, supervision; A.C.: methodology, investigation, editing, supervision; O.S.: methodology, investigation, editing, supervision; B.A.C.: data analysis, editing, review; A.C.: investigation, data analysis; C.M.P.: concept, methodology, review, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research has been carried out within the AFC PhD research program: Implications of inflammatory markers and IL-6 -597A/G and VEGF +936C/T genetic polymorphisms in chronic obstructive pulmonary disease patients profile, no. 7690/97/15.04.2016, funded through internal research programs by the “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania.
Ethical approval
Ethical approval for this study was obtained from Local Research Ethics Committee of “Iuliu Hatieganu” University of Medicine and Pharmacy Cluj-Napoca, Romania (No. 298/29.06.2016).
Informed consent
Written informed consent was obtained from all subjects before the study.