
Abstract
Spontaneous pneumomediastinum (SPM) is a rare, self-limiting condition that can be complicated by pneumothorax, pneumopericardium, and subcutaneous emphysema. This case describes a 25-year-old man with a chronic marijuana use history who developed SPM after a recent respiratory infection. Imaging showed significant pneumomediastinum, pneumopericardium, and small pneumothoraces bilaterally. Despite these findings, he remained stable and was treated conservatively with oxygen supplementation, analgesics, and close monitoring. By day 6, his condition had nearly resolved, and he was safely discharged. This case emphasizes the importance of considering SPM in young patients with acute respiratory distress and reinforces the value of computed tomography scans in promptly diagnosing and managing the condition without invasive interventions.
Introduction
Spontaneous pneumomediastinum (SPM), also known as Hamman’s syndrome, is a rare disorder characterized by spontaneous accumulation of free air in the mediastinum without trauma, iatrogenic causes, or gas-forming bacteria. 1 The incidence of SPM is estimated to be <1 in 44 000 people; it is more common in men and occurs more frequently in young adults between the ages of 20 and 30. 2 Although it is usually idiopathic, there are a variety of events that can trigger its occurrence, including but not limited to asthma exacerbations, severe coughing, vomiting, excessive physical exercise, delivery, and inhalational drugs.2,3
SPM typically presents with acute pleuritic chest pain, dyspnea, neck pain, and subcutaneous emphysema that may expand to the neck and face.1,4,5 While it is typically benign and self-limiting, it can be complicated with pneumothorax, pneumopericardium, and tension pneumomediastinum, all of which can lead to cardiovascular compromise. 6 Computed tomography (CT) is the most sensitive imaging modality used for accurate detection of mediastinal free air, even in small amounts.1,7 Management is primarily conservative, combining analgesics, oxygen supplementation, and close observation to avoid complications.2,6-8 In a few severe cases involving respiratory distress or hemodynamic instability, pleural drainage, or surgery could be relied on. 5
Case Description
A previously healthy 25-year-old male presented to the Emergency Department with complaints of shortness of breath and neck swelling following 2 days of vigorous, nonbloody, nonproductive coughing after exposure to a sick contact. The patient was in his usual state of health until 2 days before presentation, when he developed nasal congestion, nonproductive cough, and sore throat. These symptoms were similar to those of his close, sick contact. He endorsed exertional dyspnea and subjective fevers, managed with acetaminophen. Of note, the patient endorsed marijuana 3 to 4 times/day for 10 years, and that he has a sedentary job. Upon initial exam, the patient was found to be tachycardic at 106 beats/minute, hypoxic to 88% SpO2, and had leukocytosis of 17 000 WBCs. Initial neck and soft tissue X-ray imaging showed extensive subcutaneous emphysema and retropharyngeal subcutaneous gas (Figure 1). Similarly, anterior-posterior chest X-ray demonstrated extensive subcutaneous emphysema bilaterally in the right and left chest wall, extending to the left lower chest wall, as well as very small bilateral pneumothoraces (Figure 2). Subsequently, a noncontrast CT of the thorax (Figure 3a–d) revealed extensive pneumomediastinum, pneumopericardium, bilateral small pneumothoraces, and subcutaneous emphysema, prompting consultation to Cardiothoracic Surgery and Intensive Care Unit (ICU) for closer monitoring. A X-ray gastrografin esophagram (Figure 4) also ruled out esophageal injury. At this time, cardiothoracic surgery determined there was no need for a chest tube or surgery. The patient was transferred to the ICU for closer monitoring.
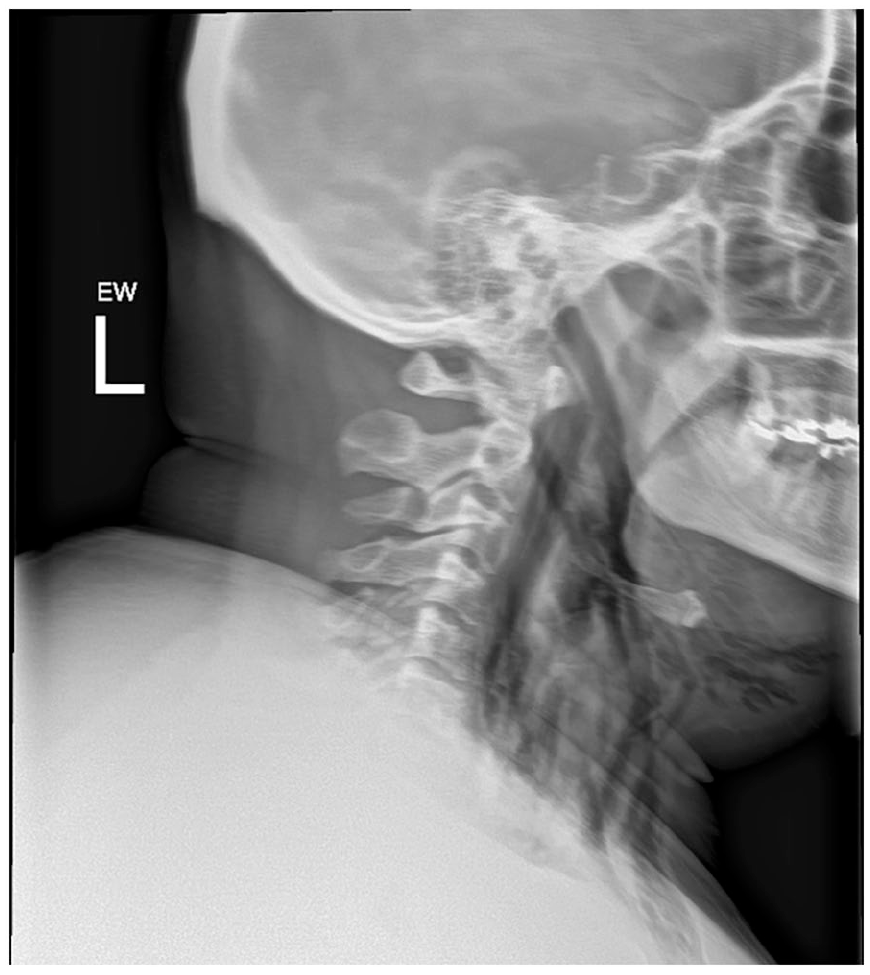
Neck and soft tissue X-ray: extensive subcutaneous emphysema and retropharyngeal subcutaneous gas.
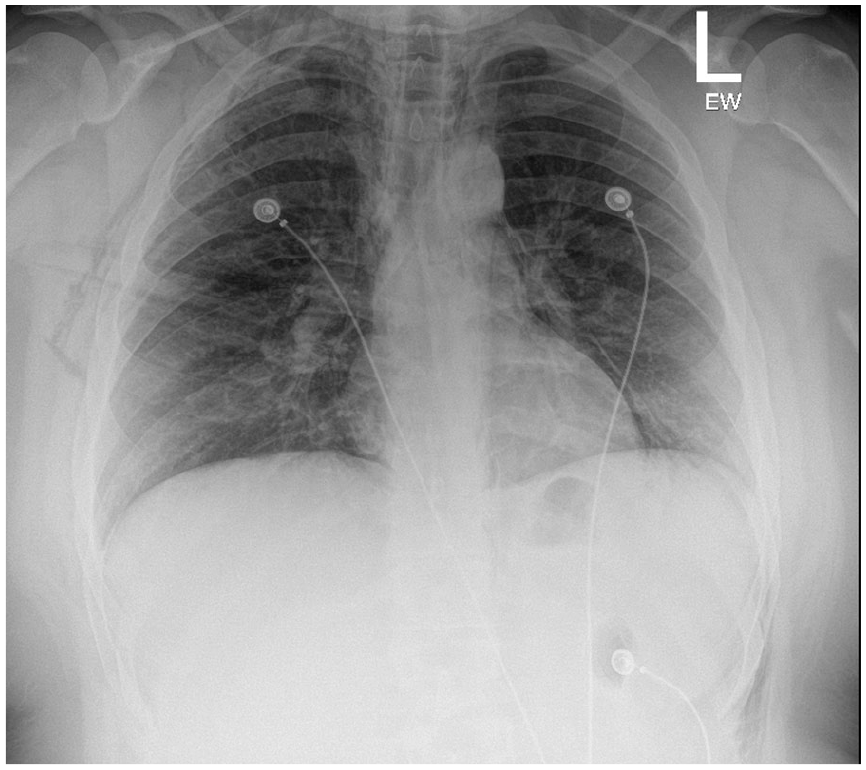
AP chest X-ray: extensive subcutaneous emphysema bilaterally in the right and left chest wall extending to the left lower chest wall.

(a) Noncontrast CT thorax: subcutaneous emphysema. (b) Noncontrast CT thorax: subcutaneous emphysema with extension to mediastinum. (c) Noncontrast CT thorax: subcutaneous emphysema with extension to mediastinum. (d) Noncontrast CT thorax: pneumpericadium and pneumomediastinum. CT, computed tomography.

X-Ray gastrografin esophagram demonstrating no extravasation of contrast.
In the ICU, the patient was hemodynamically stable and communicating without difficulty. Close monitoring for rapid expansion of pneumomediastinum while being evaluated for and/or prophylactically treated for pneumonia as a potential catalyst to the SPM. Among a variety of sputum cultures and other antigen and PCR tests, the patient was found to be positive for rhinovirus and Staphylococcus aureus in their sputum while ruling out organic causes for SPM. The antibiotics were discontinued at this time due to low suspicion of bacterial pneumonia, as the patient’s cough was nonproductive and no distinct infiltrate was appreciated on imaging. Despite a stable repeat frontal chest X-ray, the patient continued to display exertional shortness of breath and cough.
On day 3 of admission, the cough and shortness of breath were nearly resolved with only supportive care and nasal cannula oxygenation, and the patient was deemed hemodynamically stable enough to transfer to medical wards. A final repeat frontal chest x-ray on the ward showed near complete resolution of the previously identified pneumomediastinum and decreased subcutaneous emphysema in the right supraclavicular region (Figure 5). These findings were reassuring, and the patient was deemed fit for discharge.
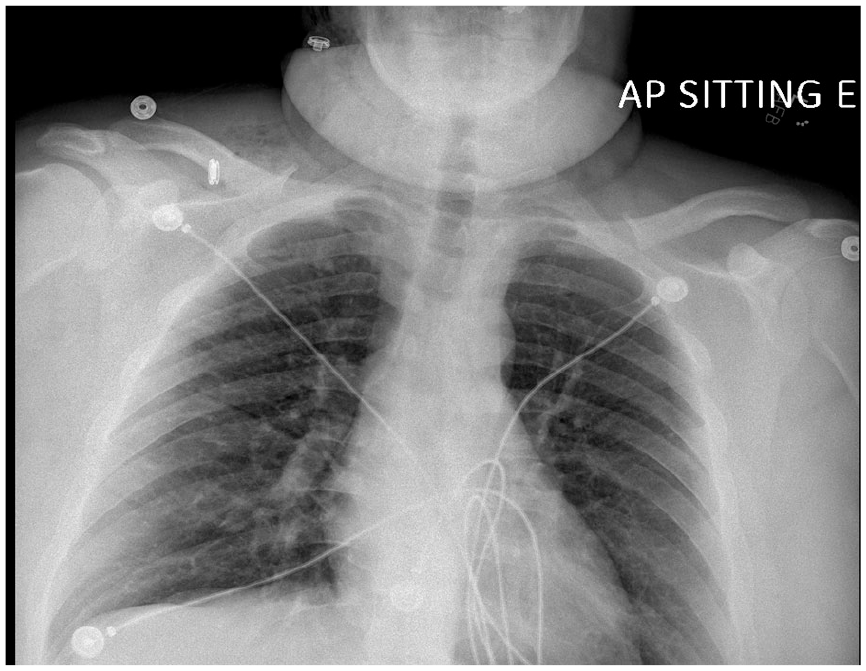
Chest X-ray on day 3: near complete resolution of the previously identified pneumomediastinum and decreased subcutaneous emphysema.
Overall, the patient was monitored, with no episodes of cardiac tamponade or escalation of care required, following a relatively benign course. Ultimately, the patient was medically stable for discharge home on day 6 of admission. The patient was discharged with an appointment for outpatient follow-up with a pulmonologist 1 to 2 weeks after discharge.
Discussion
Named after Louis Hamman, SPM is characterized by free air in the mediastinum without apparent injury.2,3,8 The phenomenon can occur when increased intrathoracic pressure, such as from a Valsalva maneuver, causes alveolar rupture and allows air to escape into the interstitial space and bronchovesicular sheaths, eventually reaching the mediastinum—this is known as the Macklin effect.3,5 SPM incidence is <1 in 44 000 people, or roughly 1 in 25 000 among younger individuals and most being male. 2 However, this frequency might be underestimated as many individuals with mild symptoms may not seek emergency care or might be misdiagnosed with muscle pain or anxiety. 2
Common presenting symptoms of SPM include, but are not limited to, chest pain, dyspnea, sore throat, and dysphagia.3,5,8 Physical examination signs such as the Hamman’s sign—subcutaneous emphysema and crunching sounds which coincide with heartbeats—can be elicited in these patients. 8 It is postulated that events that increase intrathoracic pressure, such as coughing, vomiting, defecation, childbirth, or physical activities like playing wind instruments, may be inciting events for the condition.3,5 However, spontaneous occurrence has also been documented. Interestingly, researcher Kyung Soo Kim et al reported that more than half the patients in their study did not report any of the aforementioned precipitating incidents. 5 Conversely, a different systematic review of 27 studies involving 600 patients with SPM found a predisposing factor in about one-fifth of the cases. 6 However, the most common predisposing factors were bronchial asthma, followed by interstitial lung disease, Chronic Obstructive Lung Disease, bronchiectasis, bullae, thoracic tumors, and cystic diseases.1,6
Pneumomediastinum is typically diagnosed with an anterior–posterior chest X-ray, where air outlining the mediastinal structures is the most common finding. Lateral chest X-rays are seldom necessary. Additional signs on a chest X-ray include subcutaneous emphysema, elevation of the thymus in children known as the spinnaker sign, and air surrounding the pulmonary arteries referred to as the ring sign. 7 If a chest X-ray is inconclusive, a CT scan of the chest can definitively confirm or exclude pneumomediastinum. CT scans can detect even tiny amounts of air in the mediastinum or subcutaneous tissues. They can distinguish between pneumomediastinum and pneumopericardium, a differentiation that can be challenging with a chest X-ray alone. 5
The most interesting aspect of our case was the concurrent findings of SPM and pneumothorax, pneumopericardium, and subcutaneous emphysema. Imaging showed very significant pneumopericardium, yet clinically the patient was stable throughout admission with resolution only with supportive care. The inciting event in our patient was predominantly viral pneumonia leading to an aggressive cough. It is doubtful that this was bacterial pneumonia because the patient had no infiltrative findings on CT. The patient also had a nonproductive cough, which is more attributed to viral than bacterial pneumonias. He also concurrently had a sore throat and nasal congestion, which are symptoms of viral infections. This leads us to believe these extensive radiographic findings were simply a sequel to the aggressive cough rather than a gas-forming bacterial infection. S. aureus found in the sputum was unlikely to be the culprit, as with gas-forming Staphylococcus infections, more serious disease and radiographic findings would be expected, such as necrotizing pneumonia.
Conclusion
This case highlights a rare but clinically significant SPM presentation of a young man with a chronic marijuana use history who presents with SPM after a recent viral respiratory infection. His condition was complicated by pneumothorax, pneumopericardium, and extensive subcutaneous emphysema, confirmed on CT imaging, which was essential for distinguishing SPM from other severe conditions such as esophageal rupture (Figure 4). Despite these complications, the patient was effectively treated using conservative management involving oxygen therapy, analgesia, and close monitoring. This case reinforces SPM’s early detection value, particularly in high-risk patients, and demonstrates the imaging significance in diagnosing and thorough clinical assessment in guiding appropriate management and ensuring favorable outcomes.
Footnotes
Acknowledgements
We would like to acknowledge and appreciate our patient who allowed us to publish this work in order to benefit the medical community.
Authors’ Note
A unique case of Hamman’s syndrome complicated by pneumothorax, pneumopericardium, and subcutaneous emphysema: a case report (CHEST, 166(4), A1072-A1073).
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Prior Presentation of Abstract Statement
Presented as Abstract Poster Presentation in CHEST 2024 Conference, Boston, MA, USA (October 7, 2024).