
Abstract
Diaphragmatic hernia (DH) is a condition characterized by the passage of abdominal content into the thorax. The acute symptoms associated with this entity are uncommon, pancreatic herniation being very rare. A 73-year-old patient with acute pain in the upper abdomen, distributive shock, with tomographic findings of the passage of abdominal contents into the thorax, including the pancreas, is described. The association between acute symptoms, pancreatic diaphragmatic herniation, and distributive shock is extremely rare. A case of a patient with severe acute pancreatitis secondary to DH requiring comprehensive management in the Intensive Care Unit is presented.
Introduction
Abdominal pain is responsible for 10% to 20% of emergency department visits. 1 In this syndrome, diaphragmatic hernia (DH) is an uncommon condition that requires urgent care. DH is characterized by the passage of abdominal contents into the chest through the esophageal hiatus or other congenital or traumatic orifices. 2 Different complications are associated with the presence of DH. 3 The herniated contents may consist of the gastric chamber, part of the colon, and the omentum. Pancreatic herniation is very rare, and its association with acute pancreatitis and shock is exceptional. This article presents a case of abdominal pain secondary to severe acute pancreatitis associated with acquired, nontraumatic DH, and discusses the pathophysiology of this entity.
Clinical Case
A 73-year-old female patient presented to the emergency department with 10 days of severe upper abdominal pain, intractable vomiting, diarrhea, asthenia, adynamia, and somnolence. The patient had a medical history of hypertension, chronic gastritis, Barrett’s esophagus, and DH with ambulatory follow-up. She also had a history of cholecystectomy. The patient denied alcohol consumption and reported chronic use of Valsartan 80 mg once daily, Amlodipine 5 mg once daily, and Esomeprazole 20 mg once daily. No other pharmacological treatments were reported recently.
At the physical examination, she was dehydrated and somnolent. Vital signs showed a blood pressure of 148/92 mmHg, a heart rate of 120 beats per minute, a respiratory rate of 22 breaths per minute, and a temperature of 36.7°C. No weight loss, fever, or jaundice was documented. The abdomen had no signs of peritoneal irritation, nor were masses palpable. The chest X-ray showed displacement of intestinal loops at the intrathoracic level over the right hemidiaphragm (Figure 1). Due to her worsening clinical condition, she was transferred to the Intensive Care Unit (ICU).

Chest X-ray showing intestinal contents and the gastric chamber over the right hemidiaphragm (yellow arrow).
Blood tests showed leukocytosis with neutrophils, deteriorated renal function, which required the initiation of renal replacement therapy. Liver function tests, including bilirubin levels, transaminases, and alkaline phosphatase, were within normal limits. Triglyceride and calcium levels were also within normal limits. Amylase levels were 329 UI/L and lipase levels were above 700 UI/L. Arterial blood gases with severe metabolic acidosis and an elevated anion gap (Table 1). Upon admission to the ICU, orotracheal intubation, fluid resuscitation, vasopressor support, and broad-spectrum antibiotic management were performed due to suspected abdominal sepsis. Contrast-enhanced abdominal computed tomography confirmed DH, revealing the passage of abdominal contents into the thorax, involving parts of the stomach, pancreas, and transverse colon. The pancreas showed an enlarged head and uncinate process, with adjacent fat stranding (Figures 2 and 3).
Laboratory Data..

Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; INR, prothrombin-time international normalized ratio.
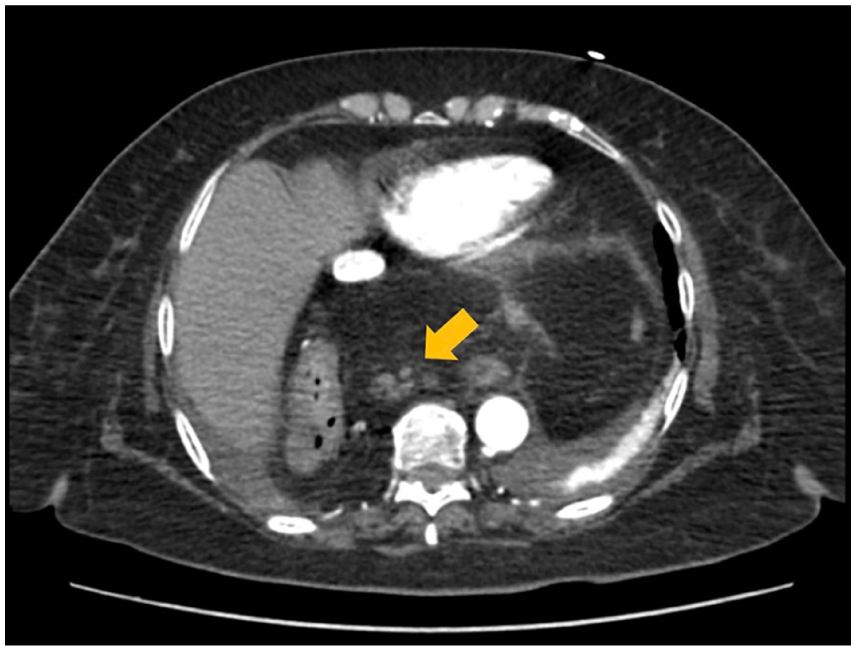
Axial section of an abdominal computed tomography scan showing a diaphragmatic hernia with herniation of the pancreas into the thoracic cavity (yellow arrow).

Coronal section of a thoracic computed tomography scan showing herniation of the stomach into the thoracic cavity and traction of the pancreas (yellow arrow).
A full study was conducted to determine the etiology of pancreatitis, ruling out alcohol, biliary, pharmacological, hypertriglyceridemia, neoplasms, autoimmune, calcium disorders, and traumatic causes. The final diagnosis was acute pancreatitis Balthazar C Marshal 9 points as a complication of DH. Surgical repair was proposed to the patient; however, the patient did not authorize the proposed procedure. Medical management included intravenous fluids, invasive mechanical ventilation and supportive care with vasopressors (norepinephrine and vasopressin) due to distributive shock, dialysis, parenteral nutrition, and sedation. Intra-abdominal pressure was managed with neuromuscular blockade and sedation. An orogastric tube and urinary catheter were also placed. After 16 days in the ICU, the patient showed satisfactory clinical improvement, with no evidence of organ dysfunction or need for further organ support and was transferred to the general ward.
Discussion
Giant HD with prolapse of the pancreas is extremely rare. 4 DH involves the passage of abdominal content into the thorax, 2 in most cases, the herniated content corresponds to the stomach, and in some less frequent cases, the colon, especially the splenic flexure.
The diagnosis of acute pancreatitis is based on the presence of 2 out of 3 criteria: (1) abdominal pain consistent with the disease, (2) elevation of serum amylase or lipase 3 times above normal values, and (3) characteristic imaging findings (pancreatic parenchymal and peripancreatic fat edema). 5 The most common etiologies are gallstones (45%) and alcohol consumption (20%), followed by less frequent causes such as autoimmunity, hypertriglyceridemia, hypercalcemia, and trauma. 5
Acute pancreatitis related to herniation of this organ through the diaphragm is a rare entity with few reports in the medical literature.6-19 The pathophysiology is still unclear, and its mechanism is probably multifactorial, with different proposed causes, including incarceration or strangulation of the hernia, ischemia related to stretching and traction of the vascular pedicle, volvulus of the biliary tree with obstruction, and repetitive trauma when crossing the hernia.6,7
The diagnosis of this entity requires a detailed clinical history, paraclinical tests and images that confirm pancreatitis, and confirmation of pancreas herniation into the thorax, ruling out other differential diagnoses.6,8 ICU integral management should be tailored according to the severity of pancreatitis. The proposed treatment ideally involves surgical repair of the diaphragmatic defect; in cases where the patient rejects the intervention or the surgical risk is high, the treatment is essentially supportive until resolution of the condition. 8
In the literature, some cases of acute pancreatitis due to HD in adults have been reported, of which most of them occurred in patients over 60 years of age.6-19 Only in 4 cases was surgical intervention reported, while in the other patients, the management was conservative with hospital discharge. This is the second report of a patient who had shock and required ICU admission and aggressive and comprehensive management.
Conclusions
Pancreatitis due to diaphragmatic herniation with ICU requirement is an extremely infrequent entity. Its diagnosis, severity, and approach require clinical expertise and ruling out other common etiologies. The definitive medical or surgical management depends on the overall context of the patient.
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval to report this case was obtained from the Ethics committee in research of the Fundacion Abood Shaio (ID approval DIB 24-07, record number 379 from February 28, 2024). This study adhered to all ethical requirements.
Consent to Participate
Written informed consent was obtained from the patient for their anonymized information, including clinical details and images, to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that clinical data are available from the corresponding author, upon reasonable request.