
Abstract
Chronic pancreatitis is commonly associated with heavy alcohol use and cigarette smoking, though many cases of chronic pancreatitis are idiopathic. Energy drink consumption has been on the rise over the last decade, with an adverse health risk profile including gastrointestinal symptoms such as dyspepsia, reflux, and gastritis. There have been several case reports linking energy drink consumption to presentations of acute pancreatitis in adult patients. To our knowledge, the association between energy drinks and episodes of chronic pancreatitis flares has not been well studied. This article explores a case of chronic pancreatitis pain related to excessive energy drink consumption in an adult male patient. This study aims to shed light on energy drinks as a potential etiology of chronic pancreatitis flares, and emphasizes the importance of counseling patients on the potential risks of excessive energy drink consumption.
Introduction
Chronic pancreatitis is a progressive disease characterized by chronic inflammation and fibrosis, resulting in functional abnormalities of the pancreas.1,2 Chronic pancreatitis most commonly occurs in male patients, and risk is higher among black patients compared to white patients. 3 Heavy alcohol use and cigarette smoking are among the most common risk factors for the development of chronic pancreatitis in adult patients, though idiopathic cases account for upward of 28% of patients with the condition.1,3 The presumed cause of idiopathic pancreatitis in adult patients is often multifaceted, with potential contributions of disease-modifying mutations and varying genetic susceptibilities in addition to environmental and behavioral components. 4 Long-term complications of chronic pancreatitis are secondary to pancreatic endocrine and exocrine insufficiency, and include diabetes, malabsorption, chronic pain, and increased risk of pancreatic cancer. 4 Several studies have also demonstrated that patients living with chronic pancreatitis report a markedly reduced quality of life with regard to physical and mental well-being.4,5 Thus, it is important to identify potential triggers of idiopathic chronic pancreatitis.
Energy drink consumption has been on the rise over the last decade. These highly unregulated beverages contain excess quantities of caffeine in addition to high concentrations of taurine, ginseng, sucrose, and B-vitamins, all of which likely contribute to their adverse health profile. There exist several reports that have explored cases of acute pancreatitis in adult patients associated with energy drink consumption,6-9 though few if any articles in our literature search have reported cases of chronic pancreatitis flares triggered by energy drink consumption. Here, we report a case of a 62-year-old man who was admitted to the hospital with a chronic pancreatitis flare after months of consuming a well-known energy drink containing 160 mg of caffeine. The patient provided informed consent for the publication of this report.
Case Report
Case Presentation
A 62-year-old male with a past medical history of chronic pancreatitis, atrial fibrillation (on Eliquis), non-ischemic cardiomyopathy (ejection fraction, 45-50%), stage III chronic kidney disease, alcohol use disorder and cocaine use disorder (both in remission), and prior cholecystectomy and gastric bypass presented to the emergency department (ED) with a four-day history of abdominal pain radiating to the lower back, nausea, vomiting, and constipation. He reported daily intermittent episodes of sharp, 10/10 abdominal pain that worsened with leaning backward and improved with sitting forward. He tolerated clear liquids but vomited solid food. Review of systems was negative for fevers, chills, cough, shortness of breath, dysuria, hematochezia, or melena.
The patient reported a remote history of cocaine use and history of heavy alcohol use, but abstained from alcohol for the past five months. He reported smoking marijuana about two to three times daily. Prior to admission, he reported drinking at least one 16-oz energy drink containing 160 mg of caffeine daily for the past several months. He feels that he “overdid it” recently, having at least two 16-oz energy drinks on the two consecutive days prior to admission. He reported feeling that these energy drinks exacerbated his abdominal pain. He denied any family history of pancreatitis or autoimmune diseases. His vital signs in the ED were as follows: temperature 98.7 ℉, blood pressure 176/102 mmHg, heart rate 79 beats per minute, respiratory rate 18 breaths per minute, and oxygen saturation of 98% on room air. On physical exam, there was tenderness to superficial and deep palpation over the left mid and lower quadrants, radiating to the lower back. His abdomen was otherwise soft and nondistended, without evidence of rebound tenderness or rigidity.
Investigations
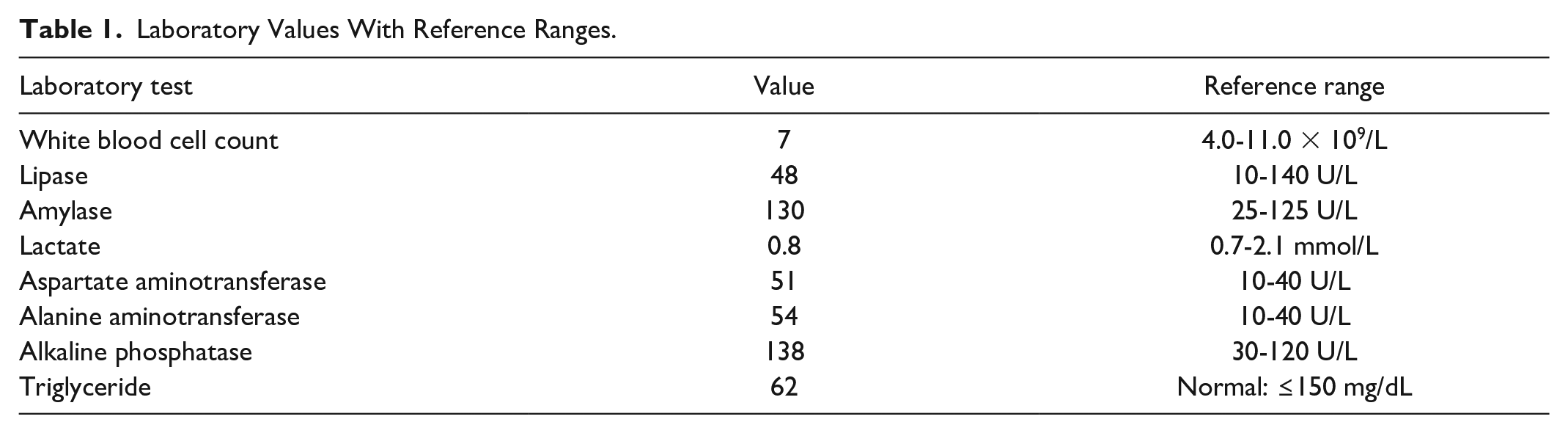
Laboratory tests collected in the ED were significant for a white blood cell count of 7 × 109/L, lipase of 48 U/L, amylase of 130 U/L, lactate of 0.8 mmol/L, aspartate aminotransferase of 51 U/L, alanine aminotransferase of 54 U/L, and an alkaline phosphatase of 138 U/L (Table 1). Chest X-ray obtained in the ED was unrevealing. Computed tomography (CT) imaging of the abdomen and pelvis did not show evidence of acute intra-abdominal pathology and reported a grossly unremarkable pancreas. Magnetic resonance imaging (MRI) of the abdomen was ordered, as it is more reliable than CT imaging or ultrasound in identifying chronic pancreatitis. 10 MRI findings consistent with chronic pancreatitis include parenchymal atrophy and main or accessory duct stenosis, stricture, or dilation. 10 In this case, MRI of the abdomen showed mild diffuse dilatation of the main pancreatic duct up to 6.4 mm in the pancreatic head, consistent with chronic pancreatitis (Figures 1 and 2). There were no changes indicative of acute pancreatitis or pancreatic head mass. Alcohol level and urine toxicology screen were negative, and his most recent triglyceride level was 62 mg/dL (Table 1).
Laboratory Values With Reference Ranges.

An axial slice of the abdomen on a half-Fourier single-shot turbo spin-echo (Haste) which is a T2-weighted sequence. It is a fluid-sensitive sequence which can be utilized for magnetic resonance cholangiopancreatography. This figure illustrates a dilated pancreatic duct in the head of the pancreas measuring 5.2 mm. No mass is visualized in the head of the pancreas. The following are the corresponding anatomic annotations. (A) Pancreatic duct, (B) common bile duct, (C) head of the pancreas, (D) superior mesenteric vein, (E) superior mesenteric artery, (F) duodenum, (G) liver.

Coronal slice of the abdomen on a Haste sequence. The image depicts a dilated pancreatic duct measuring up to 6.4 mm. Incidental note is made of a choledochal cyst which is just inferior-medial to the marker “B” in the image. The following are the corresponding anatomic annotations. (A) Pancreatic duct, (B) common bile duct, (C) pancreas, (D) superior mesenteric vein, (E) jejunum, (F) liver.
Treatment + Outcomes
The patient received intravenous fluids in the ED and was given hydromorphone and ondansetron as needed for symptom management. He was also started on a bowel regimen for management of his constipation. He was tolerant only to clear liquids for the first two days of admission, but by the third day was able to tolerate a regular diet. On the fourth day of admission after reporting adequate pain control and regular bowel movements, he was discharged home on a short course of pain medication and antiemetics as needed.
Discussion
Energy drink consumption has been on the rise over the last decade, with marketing campaigns claiming increased physical stamina, concentration, and alertness for individuals who consume these beverages. However, their use is not without risk. The association between energy drink consumption and adverse effects on the cardiovascular and central nervous system of humans has been well documented, including high blood pressure, myocardial infarction, aortic dissection, arrhythmias, sudden death, metabolic disturbances, insomnia, and seizures. 11 However, fewer studies have examined the impact of energy drink consumption on the gastrointestinal (GI) system. 11 Vague reports of GI upset have been described, in addition to several reports of dyspepsia, esophageal reflux, irritant gastritis, toxic hepatitis, and pancreatitis.6,11,12
These beverages are notoriously poorly regulated, with many containing well over the amount of caffeine deemed safe by the Food and Drug Administration (FDA) to achieve stimulatory effects.6,12-15 They also contain a variety of vitamins, minerals, amino acids, and herbal contents that are labeled as “dietary supplements” versus medications, contributing to fewer strict FDA regulations over these drinks.7,8 One 16-oz beverage of the energy drink in question contains 160 mg of caffeine. Our patient was consuming a cup of coffee in addition to at least two of these energy drinks daily, and he reported drinking more than two energy drinks on the days leading up to admission. According to the FDA, the upper limit of daily caffeine recommended in a healthy adult is 400 mg. One cup of coffee equates to roughly 95 mg of caffeine, and three of these energy drinks would equate to 480 mg caffeine, totaling about 575 mg caffeine per day. This is well above the daily caffeine limit recommended by the FDA. The exacerbation of pain in our case report, attributed to energy drink consumption, may in part be secondary to the high caffeine content of these beverages.11,16
With respect to pancreatitis, there have been several case reports that have examined energy drink consumption as a potential etiology of acute pancreatitis. A previous study by Randhawa et al 8 reported a case of acute pancreatitis in an adult patient attributed to consuming five to six energy drinks daily after conducting a thorough set of labs and ruling out biliary causes. Shmelev et al 7 further supported this association, publishing a case report featuring a patient with a remote history of acute alcoholic pancreatitis who had two episodes of interstitial edematous pancreatitis, both following consumption of Rockstar energy drinks. A study by Uwaifo reported a case of gastritis, hepatitis, and pancreatitis in a 46-year-old male with a history of well-controlled type 2 diabetes and non-alcoholic fatty liver disease who consumed two to three 16-oz cans of Monster energy drinks daily over months; dramatic improvement was noted after discontinuing the energy drinks. 6 Furthermore, the FDA’s Center for Food Safety and Applied Nutrition Adverse Event Reporting System has reported several cases of pancreatitis associated with consumption of various brands of energy drinks, including Red Bull, 5-hour Energy, Booster, and Monster Energy. 9
Several studies have explored the impact of energy drinks on the pancreas on a biochemical basis using rat models. Haroun et al 17 reported significant distortion of pancreatic cytoarchitecture upon histological examination of the pancreas in rats after ingesting energy drinks. The same was true in a study by Ayuob and ElBeshbeishy that found that energy drink consumption in rats was associated with pancreatic mucosal injury and reduced pancreatic antioxidant capacity. 18
To our knowledge, this is the first case report to examine energy drinks as a possible etiology of chronic pancreatitis flares. Patients with chronic pancreatitis often experience pain in every stage of the disease. Büchler et al 19 suggested staging chronic pancreatitis based on complications into A (early), B (intermediate), and C (end-stage) stages; our patient likely has stage A chronic pancreatitis, experiencing intermittent episodes of pain without any known significant complications. Although we cannot establish a causal relationship between energy drink consumption and chronic pancreatitis pain flares, the acute onset of pain following excessive energy drink consumption in the absence of any additional explanation for the chronic pancreatitis flare makes energy drinks the most likely cause.
Our article has several limitations. First, this is a single case report, and the generalizability of its findings is limited. Similarly, we are able to establish a correlation between energy drink consumption and chronic pancreatitis flares in this patient, but are unable to establish a cause-and-effect relationship. Next, the patient in our case report had a significant number of medical comorbidities, which may confound the association drawn between energy drinks as an etiology of his pancreatitis; however, this remains the most likely cause given his labs, imaging, and history unremarkable for other well-known causes of pancreatitis. We intend for this case report to add to the growing body of evidence surrounding the potential dangers of energy drink consumption, and the short- and long-term consequences it may have on the pancreas.
It is important for physicians to acknowledge the potential dangers of excessive energy drink consumption and counsel patients accordingly to minimize health consequences. In the future, prospective cohort studies and case series are needed to ascertain the relationship between energy drink consumption and presentations of pancreatitis.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of their patient to this study, with his case allowing them to better understand the etiology and pathophysiology of chronic pancreatitis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by the Lewis Levy, MD Student Research Fund.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.