
Abstract
Scleroderma renal crisis is a rare, life-threatening complication of systemic sclerosis. It is characterized by pronounced hypertension, acute kidney injury, and thrombotic microangiopathy. Although its prevalence has decreased over the last decade, and death rates have declined since the introduction of treatment with Angiotensin converting enzyme (ACE)-inhibitors, it remains a challenge due to lack of prevention and rapid progression despite intervention in those who develop renal crisis. We present a 46-year-old female with history of rheumatoid arthritis and scleroderma who presented to the Emergency Department (ED) with complaints of a severe headache associated with nausea and vomiting that started earlier in the day. Patient presented with a blood pressure of 180/103 that did not improve with use of anti-hypertensive medications. Labs were remarkable for anemia and decreased renal function. A CT of the abdomen and pelvis without contrast demonstrated distention of distal esophagus with possible underlying esophageal dysmotility due to degree of distention and dependent areas of tractional bronchiectasis in the bilateral lower lobes that can be seen in the setting of early interstitial lung disease. Treatment with an ACE-inhibitor was initiated, with improvement in blood pressure and resolution of headache. This case demonstrates another rare case and illustrates the importance of rapid recognition and treatment.
Introduction
Scleroderma is a rare, rheumatologic, autoimmune disorder that is characterized by fibrosis of the skin and internal organs due to excess collagen deposition.1-4 It can be divided into the localized scleroderma (only skin involved) and systemic scleroderma.1,3 The systemic form can be further divided into limited cutaneous (also known as CREST syndrome), diffuse cutaneous, sine scleroderma (no skin involvement), and overlap syndrome. 3 The most commonly affected organs include the pericardium, skin, skeletal muscle, lungs, GI tract, and the kidneys.1,3 Although signs and symptoms depend on the subtype, they include thickening of the skin, esophageal dysmotility, Raynaud phenomenon, sclerodactyly, telangiectasias, calcinosis, myalgia, arthralgia, interstitial lung disease, pulmonary hypertension, pericarditis, and scleroderma renal crisis (SRC).1,3,4 Of these manifestations, SRC is a striking and potentially fatal complication.1-5 SRC presents with new-onset or profound hypertension, acute kidney injury, thrombocytopenia, and hemolytic anemia.1,2,5,6 Patients may also present with a headache, blurry vision, or seizures.5,6 In this report, we present a rare care of SRC and highlight the importance of recognizing its signs and symptoms that would allow for prompt management.
Case Presentation
A 46-year-old female with history of rheumatoid arthritis and scleroderma who presented to the ED with complaints of a severe headache associated with nausea and vomiting that started earlier in the day. Patient reported that she receives monthly intravenous immunoglobulin (IVIG) treatment, with her last infusion the day before. She stated she woke up in the morning with a severe, diffuse headache that persisted. She reports that her blood pressure has also been elevated, but has no history of hypertension. Denied any chest pain, shortness of breath, palpitations, dizziness, lightheadedness, changes in vision, photophobia, abdominal pain, vomiting, fevers, chills, or rigor. Her scleroderma was not complicated by Raynaud’s or dysphagia. She denied any prior renal dysfunction and has never seen a nephrologist. On presentation to the ED, patient had a temperature of 98.6°F, heart rate 96 beats/min, respiratory rate 18 breaths/min, oxygen saturation 98% on room air, and blood pressure of 180/103 mmHg. Physical examination was unremarkable. Patient was not noted to have any edema, rashes, telangiectasias, skin tightening, or ulcerations.
Initial laboratory values were remarkable for BUN 18 mg/dL, Creatinine 1.60 mg/dL (with an unknown baseline renal function), albumin 2.8 g/dL, hemoglobin 9.6 g/dL, hematocrit 30.8%, platelets 116 × 103/µL, urine protein 92.7 mg/dL, and positive RNA polymerase III antibody. Laboratory values on presentation are demonstrated in Table 1. Of note, patient’s baseline renal function was unknown. Measures of inflammation and a 24 hour urine protein were not obtained. Electrocardiogram (EKG) showed normal sinus rhythm at 90 bpm without any ST segment changes. Computed tomography of the head without contrast was unremarkable. Computed tomography of the abdomen and pelvis without contrast was remarkable for distention of distal esophagus with possible underlying esophageal dysmotility due to degree of distention (Figure 1), and dependent areas of tractional bronchiectasis in the bilateral lower lobes that can be seen in the setting of chronic aspiration or early interstitial lung disease (Figure 2). Patient was initially treated with Labetalol 15 mg and Clonidine 0.1 mg without any significant improvement in her blood pressure. After receiving both medications, repeat blood pressure was 170/101 mmHg. Primary team began hypertension management with Carvedilol 6.25 mg twice a day and a 1-time dose of Nifedipine 30 mg.
Laboratory Values From Day of Presentation.


Computed tomography without contrast demonstrating dilation of distal esophagus (blue arrow).
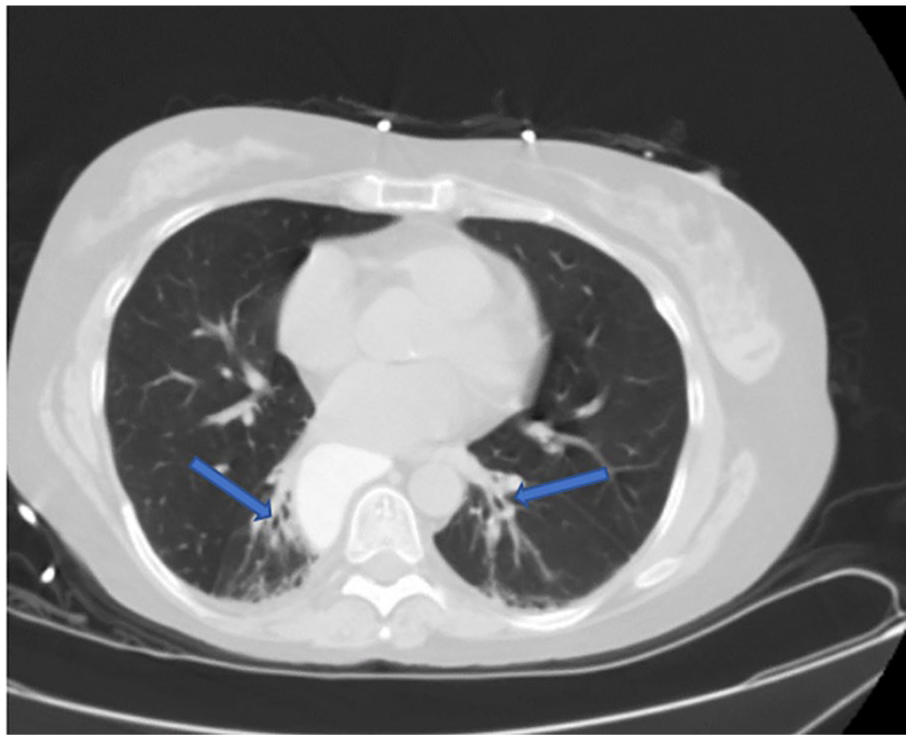
Computed tomography without contrast showing areas of tractional bronchiectasis in the lower lobes (blue arrows), most likely due to early interstitial lung disease in setting of systemic scleroderma.
Nephrology was consulted due to her medical history of scleroderma, who were concerned for potential renal crisis in setting of thrombocytopenia, anemia, and hypertension, with recommendations for further hematologic evaluation, renal Doppler ultrasound to evaluate for renal artery stenosis, and initiation of captopril 12.5 mg 3 times daily for treatment of SRC. Hematologic evaluation for potential source of hemolytic anemia was negative. Renal Doppler ultrasound was unremarkable.
Following treatment with captopril and carvedilol, her blood pressure began improving (Table 2), with systolic blood pressures (SBP’s) dropping as low as 110’s. Patient also reported improvement in her headaches. Carvedilol was discontinued, and captopril was switched to ramipril 5 mg daily, and eventually increased to 10 mg daily. Over the course of the hospital stay, her SBP ranged from 120 to 150’s with resolution of the headache. Renal function remained stable (Table 3). Patient was discharged 2 days after admission per her request. She was advised to follow-up with nephrology on discharge for further work-up of her proteinuria and potential renal biopsy.
Blood Pressure Log Over Course of Hospital Stay Also Noting Time of Medication Initiation.

Renal Function Over Course of Hospital Stay.

Discussion
Systemic sclerosis (SSc) most commonly affects women of childbearing age, with a female to male ratio of 5 to 1. 1 African Americans have an increased risk of developing SSc have an earlier age of onset, between 45 and 54, and tend to have more severe disease. 1 Genetic factors, such as human leukocyte antigen (HLA) antigens, as well as environmental factors, such as exposure to infectious agents, organic solvents, and smoking have been theorized to be risk factors for its development. 1 Autopsy studies have demonstrated renal involvement in 60% to 80% of individuals with SSc.2,6 The different forms of renal involvement include antiphospholipid associated nephropathy, Anti-Neutrophil Cytoplasmic Antibodies (ANCA) associated vasculitis, membranous nephritis, isolated reduced glomerular filtration rate, high intrarenal arterial stiffness, and proteinuria.2,6 Of these forms, SRC is potentially fatal. 6
SRC is the most serious manifestation of SSc.1,6 It is seen in close to 10% of individuals with scleroderma. 2 It is usually seen within the first 3 years of diagnosis, and a median duration of 7 months from the first non-Raynaud manifestation.1,6 A number of risk factors have been identified for its development, including steroids (especially in high doses), new onset anemia, presence of anti-RNA polymerase III antibody, prior use of cyclosporine, SSc for more than 4 years, tendon friction rubs, and new onset pericardial effusion or heart failure.1-3,6 Of those, the most important is widespread skin involvement, particularly if it is rapidly progressing.2,6
Although the pathogenesis of SRC has yet to be clearly defined, it has been hypothesized that the primary insult involves injury to endothelial cells, with subsequent intimal thickening and proliferation of the arcuate and interlobular renal arteries. 4 Platelet factors additionally prompt further lumen narrowing through collagen formation, fibrin deposition, and increased vascular permeability. 2 This in turn results in decreased arterial blood flow, which causes amplification of the renin–angiotensin–aldosterone system due to hyperplasia of the juxtaglomerular cells, resulting in accelerated hypertension.4,5 Renal biopsy will reveal endothelial damage and thrombus formation, particularly small vessel thrombosis. 2 Due to its predominant small vessel involvement and intimal thickening that causes lumen obliteration, it results in an “onion skin” appearance histopathologically.2,5
The presentation of SRC varies and its diagnosis is clinical. On initial evaluation, SRC should be considered in all patients with an acute increase in blood pressure and acute kidney injury.5,6 Kidney biopsy is not required, but may be useful in ruling out other diagnoses. 6 Although no clear guidelines for diagnosis have been defined, the Scleroderma Clinics Trials Consortium have worked on identifying a clear-cut set of variables that are currently being utilized. 5 These variables include blood pressure, kidney injury, organ dysfunction, histopathology, microangiopathic hemolytic anemia, and thrombocytopenia. 5
An acute increase in blood pressure is defined as a patient presenting with a SBP of 140 mmHg or higher, diastolic blood pressure (DBP) of 90 mmHg or higher, an increase in SBP of 30 or more above baseline, or an increase in DBP of 20 or more above baseline. The blood pressure measurements should be taken 2 times, separated by at least 5 minutes, and should be taken until consistent readings are obtained. The definition for acute kidney injury follows the kidney disease improving global outcomes (KDIGO) guideline. This includes an increase in serum creatinine of 0.3 mg/dL or more within 48 hours, increase in serum creatinine 1.5 times or more from the patient’s baseline presumed to have happened within the last 7 days, or urine volume less than 0.5 mL/kg/h for 6 hours.2,5
Microangiopathic hemolytic anemia presents with new or worsening anemia not related to other causes, schistocytes or other red blood cell fragments on peripheral smear, laboratory evidence of hemolysis such as elevated lactate dehydrogenase/reticulocytotis/low or absent haptoglobin, and a negative direct antiglobulin test. Thrombocytopenia is seen with a platelet count of 100,000 or less that must be confirmed with a manual smear.2,5
Organ dysfunction is defined as hypertensive retinopathy (cotton wool exudates, disk edema, hemorrhage), acute pericarditis, acute heart failure, or hypertensive encephalopathy (headache, seizures, altered mental status). Histopathology findings in SRC include small vessel changes, glomerular changes of thrombotic microangiopathy, nonspecific ischemic changes of the glomerular basement membrane, early vascular changes (thrombosis, fibrinoid necrosis, accumulation of myxoid material), narrowing and obliteration of the vascular lumen, glomerulosclerosis, and the classic “onion-skin” lesions.2,5
In patients with high-risk features, such as presence of anti-RNA polymerase III, acute kidney injury within 5 years of diagnosis, glucocorticoid use in the past 6 months, and skin involvement, the diagnosis of SRC can be established with the presence of blood pressure and acute kidney injury as defined above. In those without high-risk features, diagnosis of SRC requires the addition of one of other variables mentioned. 6 As far as glucocorticoids, it has previously been noted that the mechanism for increasing risk is by inhibiting prostacyclin production along with induction of ACE activity. 5
The treatment of SRC involves hospitalization, early and aggressive therapy for rapid treatment of blood pressure, and involvement of the nephrology team. Early treatment is crucial to prevent further complications of SRC. 2 The primary endpoint of treatment is to return the patient back their baseline blood pressure within 72 hours and to prevent irreversible kidney damage. First-line therapy for SRC is an ACE-inhibitor, which should be started once the diagnosis is established. In individuals with a SBP of less than 180 mmHg or DBP of less than 110 mmHg, it is optimal to start the ACE-inhibitor alone, with the goal being to reduce the SBP by 20 mmHg or DBP by 10 mmHg per day. Captopril is the preferred agent due to its shorter half-life and rapid onset of action. However, ramipril has also been used. If treatment remains suboptimal after the use of the maximal dose, additional therapy with other anti-hypertensives should be utilized, such as calcium channel blockers, angiotensin receptor blockers, and alpha-blockers. Beta-blockers are avoided, as it results in increased peripheral resistance and vasoconstriction. If the blood pressure is greater, one should consider admission to the critical care until and starting intravenous anti-hypertensives. One should also be aware that although ACE-inhibitors may further deteriorate renal function, treatment should be continued, as renal function may rebound. As for long-tern management, ACE-inhibitors should be continued, even if patients are dialysis-dependent, as it may improve chances of becoming dialysis-independent. The exact mechanism to which ACE-inhibitors manage SRC has yet to be understood.2,4-6
Several studies that have used ACE-inhibitors in patients with SSc prior to the development of SRC did not show any benefit. In fact, prophylactic use of ACE-inhibitors was associated with a higher incidence SRC and a worse prognosis.2,3
In the case that we present, the patient met the criteria for diagnosis of SRC based off the variables described by the Scleroderma Clinics Trials Consortium. Blood pressure on presentation was 180/103 mmHg. Creatinine was 1.60 mg/dL. Although we do not know her baseline renal function, it most likely met the KDIGO guideline given being a young age and no prior history of kidney disease. Patient also presented with normocytic anemia, which may be new or worsening, given no prior labs were available. RNA polymerase III antibody was also positive, placing the patient at a higher risk for development of SRC. With the use of captopril, which was eventually switched to ramipril, patient’s blood pressure gradually improved, as well as the renal function. This provides further evidence of the importance of rapid treatment and the utilization of ACE-inhibitors.
Conclusion
SRC is a rare and potentially fatal complication of SSc. In our case, treatment with captopril and ramipril was rapidly initiated, allowing for gradual improvement in blood pressure and renal function. This highlights the importance of rapid recognition of potential signs and symptoms, as well how treatment with ACE-inhibitor is crucial to prevent irreversible kidney and potential death.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.