
Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most prevalent and aggressive subtype of non-Hodgkin lymphoma comprising 30% to 40% of cases. While DLBCL frequently arises in the lymph nodes, up to 40% of cases originate in extranodal tissues. Primary splenic DLBCL is extremely rare comprising only ~1% of DLBCL cases and can be complicated by rare entities including gastrosplenic fistula (GSF). In contrast to DLBCL, polycythemia vera (PV) is a myeloproliferative malignancy. Polycythemia vera can transform into other hematologic malignancies including post-polycythemia myelofibrosis, but associations with DLBCL are uncommon. We present the first case of PV with concomitant primary splenic DLBCL complicated by GSF. While the majority of splenic lesions are benign, they have a broad differential diagnosis including malignant etiologies. Cystic or solid morphology, the number of lesions, and vascularity on imaging heavily guide further management. Due to concern for imminent massive upper gastrointestinal bleeding in the setting of GSF, our patient was diagnosed and managed with prompt splenectomy and gastrectomy. Percutaneous splenic biopsy is also a safe and effective diagnostic modality, but was deferred in our case given increased bleeding risk with PV. In conclusion, primary splenic lymphoma should be in the differential for a splenic mass regardless of whether the patient has a prior hematologic malignancy, and management should be prompt especially if complicated by a GSF.
Keywords
Introduction
Non-Hodgkin lymphoma (NHL), the most common hematological malignancy with 77 240 new cases in 2020, can have a poor survival rate depending on the type and associated aggressiveness, stage, patient factors, and management implemented.1-3 Specifically, NHL arises from precursor or mature B lymphocytes, including plasma cells, and T lymphocytes, where the former comprises the majority (85-90%) of cases. 4 Diffuse large B-cell lymphoma (DLBCL) is the most aggressive and prevalent NHL subtype in adults making up approximately 30% to 40% of total cases. 3 Indeed, although the overall 5-year survival rate for DLBCL can differ depending on various factors, it is estimated to be around 60% but can drop to the 20s for higher risk disease.5,6
While DLBCL most commonly arises in the lymph nodes, up to 40% of cases can originate in extranodal tissues with the most frequent primary location being the stomach and intestines. 7 Other frequent locations of primary extranodal DLBCL includes the central nervous system, testis, thyroid, and nose/sinuses. 7 Conversely, primary splenic DLBCL is extremely rare comprising only ~1% of DLBCL cases. 8 Additionally, primary splenic DLBCL may be complicated by rare entities including gastrosplenic fistula (GSF) formation. Indeed, the most common etiology of GSF is splenic DLBCL. 9 In contrast to DLBCL which is a lymphoid neoplasm, polycythemia vera (PV) is a myeloid neoplasm, specifically a myeloproliferative malignancy. While PV can transform into other hematologic malignancies including post-polycythemia myelofibrosis, acute myelogenous leukemia, or myelodysplasia, associations with DLBCL are uncommon. Here, we present an exceptionally rare case of PV with concomitant newly diagnosed primary splenic DLBCL complicated by GSF.
Case Report
A 72-year-old male with a history of JAK2 V617F–positive PV with possible early post-polycythemia myelofibrosis presented due to left upper quadrant (LUQ) abdominal pain for 3 months, and recent imaging findings of a splenic mass with possible GSF. He also reported 30 lb weight loss, early satiety, poor appetite, and fatigue during this time. Three months prior to presentation, for his symptoms, he underwent computed tomography of the abdomen and pelvis (CT A/P) locally which revealed a 10.7 × 9.7 × 13.6 cm predominantly cystic/solid splenic mass; hematoma, malignancy, or an abscess was considered, where the latter was thought to be less likely. Repeat CT 3 months after showed an enlarging splenic mass (14 × 11.5 × 15.4cm) with perisplenic stranding concerning for possible tumor spread or evolving rupture. For further characterization, a Positron Emission Tomography (PET)-CT was performed 1 week later revealing a hypermetabolic, locally invasive, large necrotic splenic lesion with extensive hypermetabolic upper abdominal lymphadenopathy as well as a sternal lesion which were suspicious for malignancy. There was also concern for possible GSF but this was uncertain on the noncontrast CT prompting hospital admission for further workup. He denied fever, chills, night sweats, headaches, vision changes, nausea, emesis, bleeding or easy bruising, blood in the stool, changes in bowel habits, and family history of cancer or bleeding disorders.
His vital signs were normal and on examination he appeared fatigued. Abdominal exam revealed significant splenomegaly with masses appreciated on palpation. He also had LUQ pain on palpation. The remaining exam was overall unremarkable. Labs revealed microcytic anemia with a hemoglobin of 9.5 (previously 10-11), thrombocytosis (422; previously in the 400s) and leukocytosis (18.1; neutrophils 15.36, lymphocytes 0.84). Liver chemistries were elevated including alanine aminotransferase (ALT, 127), aspartate aminotransferase (AST, 95), and alkaline phosphatase (351; previously in the 150s) with a normal total bilirubin. CT angiogram of the A/P revealed a large centrally necrotic process in his spleen filled with gas and fluid measuring 14 × 11.5 × 15.4 cm with communication with the lumen of the greater curvature of the stomach but without stigmata of active bleeding (Figure 1). This GSF was new compared to the CT performed 1 week prior. Imaging also revealed presumed malignant abdominal and retroperitoneal lymphadenopathy as well as a splenic artery aneurysm measuring 0.9 cm.
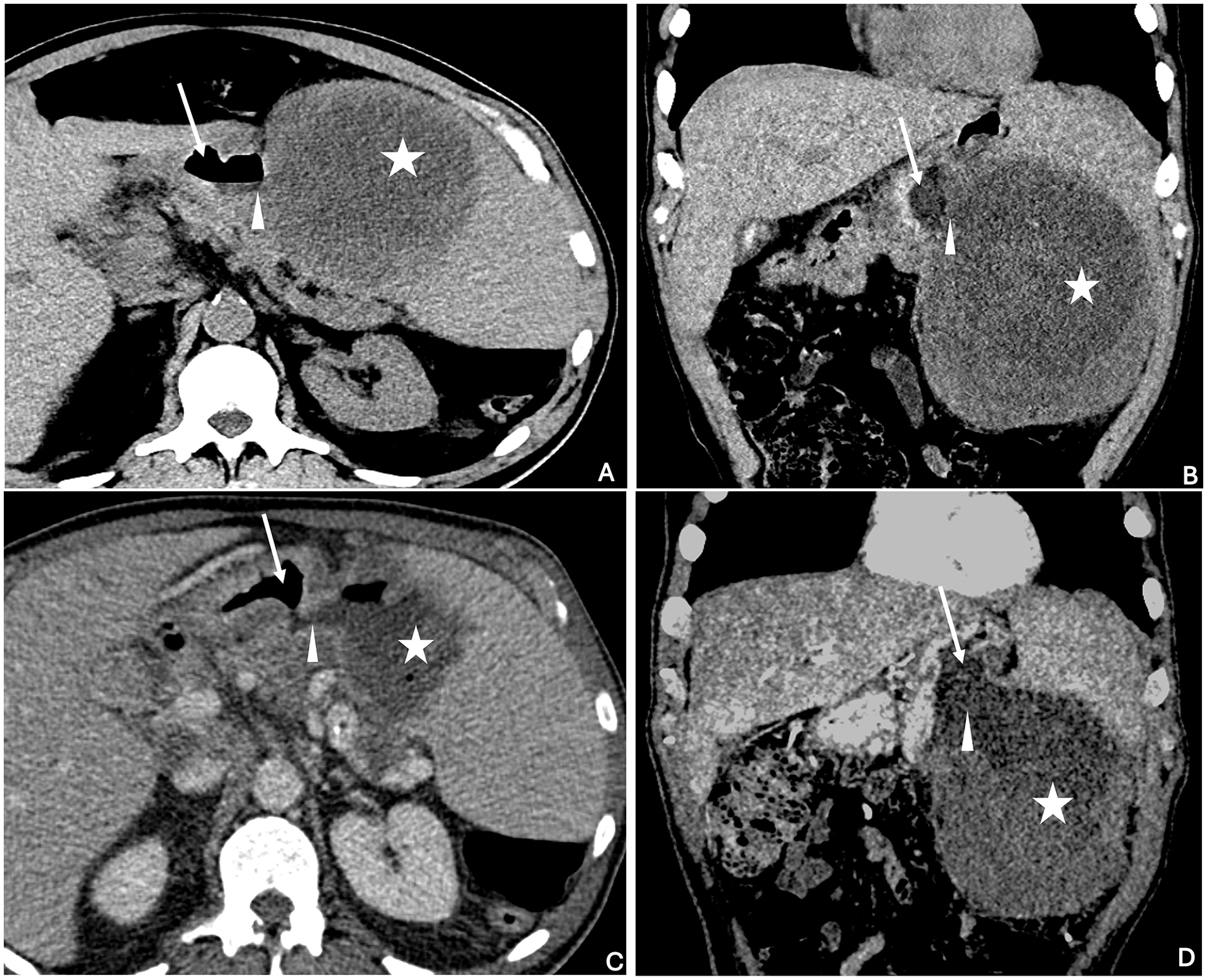
Noncontrast axial (A) and coronal (B) CT images demonstrate a large hypoattenuating mass in the spleen (star). Gas is seen within the lumen of the gastric body (arrow), and not within the splenic mass. However, the gastric wall between the mass and gastric lumen is nearly imperceptible (arrowhead). Contrast-enhanced axial (C) and coronal (D) CT images demonstrate a definite defect in the gastric wall (arrowhead) between the gastric lumen (arrow) and splenic mass (star). Gas is now seen within both the gastric lumen and the splenic mass.
Hematology and surgery were consulted for possible primary splenic lymphoma complicated by GSF. Given concerns for eventual massive upper gastrointestinal bleeding (UGIB), the patient underwent prompt splenectomy, gastrectomy, and distal pancreatectomy due to dense adherence to the pancreas. Intraoperatively, the splenic mass measured 17 cm in maximum dimension. Bone marrow biopsy was negative for lymphoma involvement. Surgical pathology showed DLBCL prompting treatment with rituximab, high-dose steroids, and chemotherapy (Pol-R-CHP) within 2 weeks postoperatively. After undergoing 3 cycles of chemotherapy, on PET-CT 3 months after admission, there was resolution of the previously seen abdominal lymphadenopathy.
Discussion
In the United States, approximately 28 000 annual admissions to the hospital are related to enteric fistulas and similarly, hematologic malignancies contribute to 20.2% of all malignancy-related hospitalizations.10,11 We however present a unique case, the first to our knowledge, with two hematologic malignancies, one which was newly diagnosed and complicated by GSF formation. Indeed, while an extensive literature search in PubMed/Medline and Embase since inception did reveal a few reports of concomitant PV and DLBCL in general, there were no other cases of PV and primary splenic DLBCL with GSF.
The spleen is the largest secondary lymphoid organ and is composed of two major tissue types including the red pulp and white pulp, where the former contains vascular structures and latter consists of the lymphatic tissue. 12 Correspondingly, most splenic lesions are of vascular or lymphatic origin. 12 In contrast to our case, splenic lesions are typically found incidentally in asymptomatic patients where imaging characteristics are heavily relied upon to determine the direction of further workup and management. 12 While the majority of splenic lesions are benign, specifically hemangiomas, it is important to be aware of and rule out malignant etiologies including primary splenic lymphoma, sarcoma, and metastasis if there is high clinical suspicion.12,13 Splenic lesions can be categorized first on whether the mass has a cystic, solid, or combination radiologic appearance, and subsequently by whether it is solitary or numerous. Solid lesions can be further subdivided based on vascular or non-vascular origin.12,13 These are however general classifications, and morphology on imaging may not completely exclude a specific type of lesion. The differential diagnosis for splenic lesions is summarized in Table 1.12,13 In our case, there was some discrepancy between radiologists on whether the initial CT A/P demonstrated a cystic mass or a predominantly cystic mass with a solid component.
Differential Diagnosis of Splenic Lesions.

Based on the imaging but also the clinical presentation, the differential diagnosis for the splenic mass initially for our patient consisted of abscess, hematoma, second primary malignancy including lymphoma, and PV-associated splenomegaly due to extramedullary hematopoiesis or splenic infarctions. Given no signs of infection or recent known trauma, abscess and hematoma were thought to be less likely. Conversely, given the patient’s symptomatology including weight loss, fatigue, early satiety, and imaging demonstrating extensive upper abdominal lymphadenopathy and a sternal lesion, a malignant etiology was highest on the differential. Similarly, a splenic primary malignancy was suspected rather than metastasis from another location given that the PET-CT did not reveal a distant primary neoplasm. Additionally, given the presence of a new GSF, a rare entity with a relatively narrow differential diagnosis (Hodgkin lymphoma, NHL, gastric adenocarcinoma, metastasis to stomach, peptic ulcer disease, splenic abscess, Crohn’s disease, bariatric surgery, trauma), primary splenic lymphoma was highest on the differential given that NHL is the most common etiology. 9
Depending on the suspected identity of the splenic mass based on imaging, a tissue sample may or may not be necessary for definitive diagnosis.12,13 If the diagnosis is uncertain on imaging, tissue sampling is warranted.12,13 Specifically, tissue sampling can involve percutaneous image-guided biopsy, or total or partial splenectomy. Notably, percutaneous image-guided biopsy has been avoided historically due to concerns of hemorrhage and low diagnostic yield. However, a meta-analysis of percutaneous image-guided biopsy has demonstrated high diagnostic accuracy (sensitivity = 87%, specificity = 96.4%) and a low major complication rate of 2.2% which is comparable to that reported for liver and kidney biopsy.12,14 For our patient, as primary splenic lymphoma was the highest on the differential, and given that the situation was complicated by the GSF, we opted for splenectomy as this would be both diagnostic and therapeutic. Additionally, given the concomitant PV and dysfunctional platelets, as well as the presence of the splenic artery aneurysm, our patient was at a higher bleeding risk prompting us to avoid biopsy.
One major strength of our case was that the patient underwent prompt splenectomy and gastrectomy given the new GSF, decreased hemoglobin, and risk for massive UGIB. 9 If the patient did present with a massive UGIB, he would likely require emergent interventional radiology–guided embolization of the splenic artery. One limitation of our case was that although we planned to avoid initial empiric chemotherapy postoperatively to prevent impaired wound healing, the subsequent histopathological diagnosis of DLBCL required us to start chemotherapy only 2 weeks after surgery. This paper was formatted according to the CARE guidelines for case reports. 15
In conclusion, here we present an extremely rare case of PV with concomitant newly diagnosed primary splenic DLBCL complicated by GSF. Primary splenic lymphoma should be in the differential for a splenic mass regardless of whether the patient has a prior hematologic malignancy, and management should be prompt especially if complicated by a GSF.
Footnotes
Author Contributions
Bibek Saha: Conceptualization, data extraction, writing—original draft, writing—review & editing final manuscript.
Jenny J. Cao: Writing—review & editing final manuscript.
Zachary S. Kelm: Data/image extraction, writing—review & editing final manuscript.
Allison Reinhardt: Writing—review & editing final manuscript.
Alex Danielson: Writing—review & editing final manuscript.
Victoria Kalinoski-DuBose: Writing—review & editing final manuscript.
William Mundell: Writing—review & editing final manuscript, supervision.
Data Availability Statement
Data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
All patient information has been de-identified. Written informed consent was obtained from the patient for their de-identified information to be published.
Submission Declaration and Verification
This manuscript has not been published previously or in a different language. Additionally, this manuscript is not simultaneously being submitted for publication elsewhere and is not currently under consideration at a different journal. An abstract of this case is currently under review for poster presentation at SGIM 2025. The publication of this manuscript is approved by all authors. If this manuscript is accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.