
Abstract
Neuroendocrine cells are distributed throughout the body’s organs, though neuroendocrine neoplasms are primarily documented in the gastrointestinal tract and pancreas, with rare occurrences elsewhere. Herein, we report a case of primary neuroendocrine tumor of the omentum (omental NET) that was incidentally detected as an omental mass during preoperative screening for colorectal cancer. The patient, a 66-year-old woman, with abdominal pain and decreased oral intake, leading to a diagnosis of obstructive colorectal cancer with a large, 55 mm, mass around the gastropyloric region, which was discontinuous with the gastrointestinal tract. After the placement of a colonic stent at the site of the ascending colon cancer to decompress the colon, a laparoscopic right hemicolectomy was performed, simultaneously excising the mass. Postoperative pathology revealed a neuroendocrine tumor (NET). Subsequent examinations detected no other lesions of suspected primary disease and postoperative somatostatin scintigraphy found no other lesions, establishing a diagnosis of omental NET. The rarity of omental NETs is attributable to the absence of neuroendocrine cells in the omentum. Moreover, solid tumors originating primarily from the omentum are very rare, making preoperative diagnosis difficult; therefore, postoperative pathology should be utilized. We presented a very rare case of omental NET, previously reported only once in the literature, and believe that complete resection with minimal invasiveness should be performed for treatment of this malignancy. In addition, we emphasize the need for continued patient follow-up.
Introduction
Neuroendocrine cells are present in all organs; however, neuroendocrine neoplasms (NENs) occur mainly in the gastrointestinal tract and pancreas and rarely in other parts of the body.1,2 Among them, those that occur in the omentums are extremely rare, with only 2 cases, including the present case. Herein, we report a case of primary neuroendocrine tumor of the omentum (omental NET) that was incidentally discovered as an omental mass during preoperative screening for colorectal cancer.
Case Presentation
A 66-year-old woman complained of abdominal pain and decreased oral intake, leading to a diagnosis of obstructive colorectal cancer.
Incidentally, a noncontiguous mass was detected around the gastropyloric region on computed tomography (CT), suggesting lymph node metastasis of the ascending colorectal cancer and gastrointestinal stromal tumor (Figure 1).
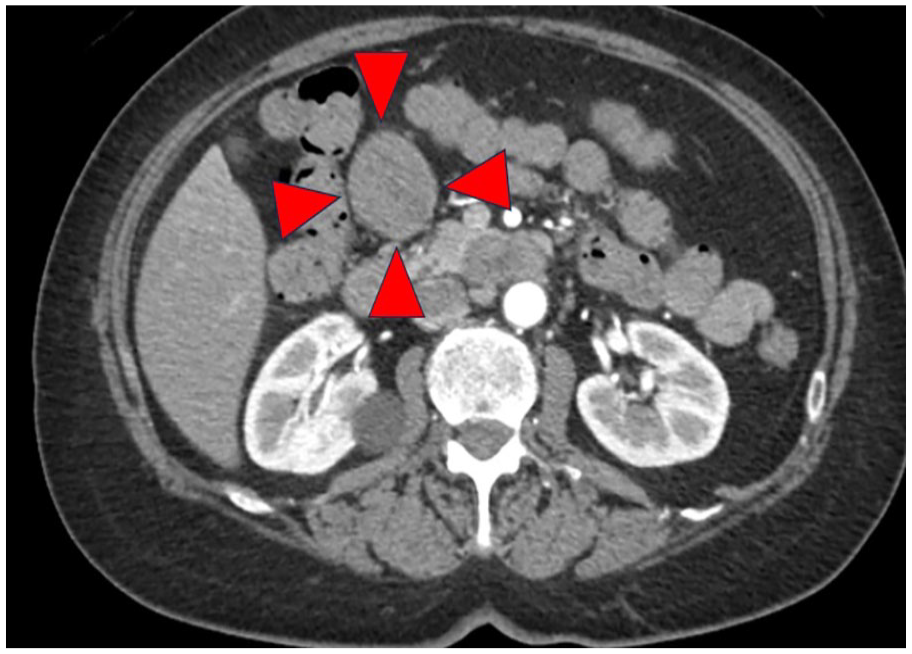
A noncontiguous mass was detected around the gastropyloric region on computed tomography.
The patient had an unremarkable personal and fam-ily medical history, and she was not taking any notable medications.
Her physical examination revealed mild abdominal distension with no palpable mass. Clinical examination revealed anemia but the tumor markers (such as CEA and CA19-9) were not elevated. T2-weighted magnetic resonance imaging (MRI) showed high signal intensity with internal heterogeneity, and diffusion-coordinated MRI was high (Figure 2a, b). Upper gastrointestinal endoscopy did not identify any neoplastic lesions, while endoscopic ultrasonography (EUS) detected a 55 mm diameter lesion in the perigastric region. NET was detected in EUS-guided fine-needle aspiration (Figure 3).
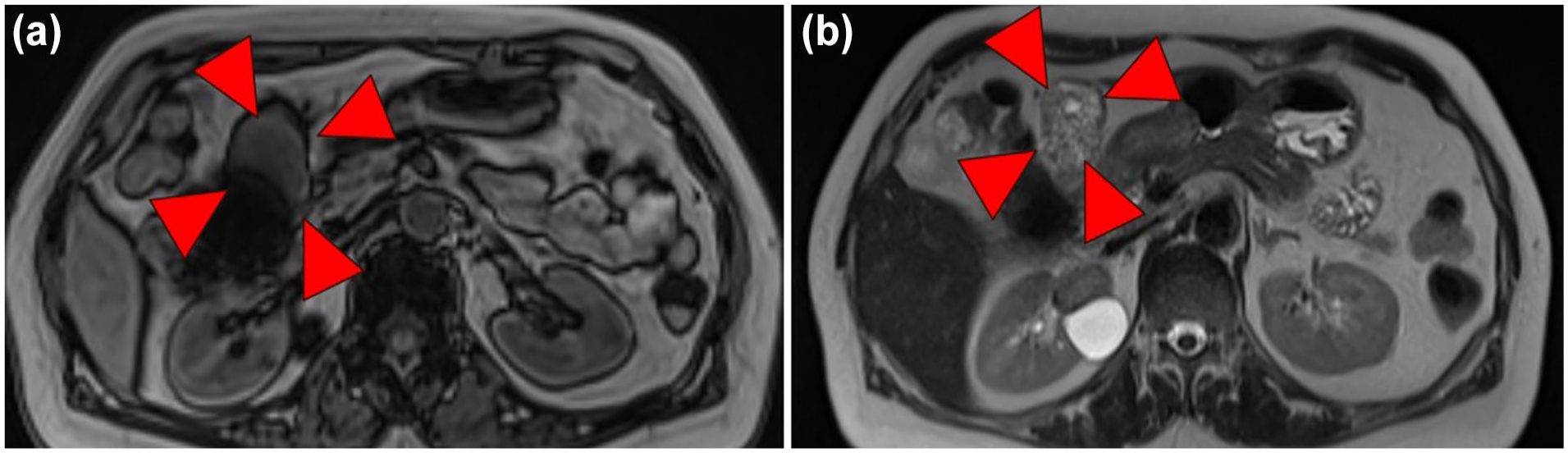
(a, b) T2-weighted MRI showed high signal intensity with internal heterogeneity and diffusion-coordinated MRI was high. MRI, magnetic resonance imaging.

Endoscopic ultrasonography detected a 55 mm diameter lesion in the perigastric region.
Laparoscopic surgery was performed after intestinal decompression by placing a colonic stent at the site of the ascending colorectal cancer lesion. The patient was placed in the lithotomy position under general anesthesia combined with epidural anesthesia, and a laparoscopic right hemicolectomy was performed. The tumor was located in the greater omentum along the right gastroepiploic artery and vein, with no continuity with the gastrointestinal tract. Other than the tumor, there were no obvious nodes suspicious for extra-regional lymph node metastasis, an atypical finding for lymph node metastasis. Therefore, we decided to resect the tumor individually.
After colon resection, sharp dissection was performed using the Harmonic 1100i™ shears (ETCHICON Inc., Raritan, NJ), and the tumor was excised without resecting the surrounding blood vessels (Figure 4).

The tumor existed separately from the surrounding blood vessels.
Histologically, NET was diagnosed based on the presence of numerous pseudorosettes of cells with a high nucleocytoplasmic ratio (Figure 5a); positivity for chromogranin A (Figure 5b), synaptophysin (Figure 5c), and CD56 (Figure 5d); and negativity for CEA. Ki-67 positivity ranged from 3% to 5%, corresponding to NET-G2.

Low-power field. (a) HE staining. The tumor showed pseudorosette arrangements and had high nucleocytoplasmic ratios. (b) Expression of chromogranin was observed in cells. (c) Expression of synaptophysin was observed in cells. (d) Expression of CD56 was observed in cells.
The postoperative course was uneventful, and the patient was discharged on postoperative 12 days. Capecitabine and oxaliplatin were administered as postoperative adjuvant chemotherapy for colorectal cancer during the first 6 months postoperatively. At 12 months later, there was no evidence of recurrence or metastasis.
Postoperative somatostatin receptor scintigraphy (SRS) did not reveal any suspicious lesions. Therefore, finally, we diagnosed omental NET as the primary lesion.
Discussion
NETs arising in the gastrointestinal tract are relatively rare, with a reported annual incidence of 3.5 per 100,000 people. Most frequently, such tumors occur in the pancreas and gastrointestinal tract. 3
Ultrasonography, CT, MRI, ¹⁸F-fluorodeoxyglucose-positron emission tomography (¹⁸FDG-PET), and SRS are recommended to locate metastases in NEN,3-7 and appropriate tests should be selected and performed based on the individual clinical situation. Unfortunately, we would not perform ¹⁸FDG-PET in this case.
The SRS test, which is used to detect many neuroendocrine cell types expressing somatostatin receptors, has a reported sensitivity and specificity of 52% and 93%, respectively. It is useful for detecting NENs because it allows whole-body scanning and detects somatostatin receptor expression.
Several possible etiopathogenic mechanisms exist, similar to those observed in rare NETs such as NETs of gallbladder8,9 or primary hepatic NETs.10,11 These mechanisms include tissue changes arising from stem cells or undifferentiated cells,8,9 transformation of neuroendocrine cells in lymph nodes,12-14 development due to a change in the direction of differentiation during the growth of malignant tumors,15-18 and ectopic origins from pancreatic or adrenal tissue. 19 In the present case, there was no obvious adenocarcinoma or ectopic tissue within the tumor, and it was highly likely that the tumor arose by differentiation from undifferentiated cells or by plasmatic transformation.
Although guidelines for nonfunctioning NETs consider surgical resection due to malignant potential, for example, when the tumor diameter exceeds 1 cm or shows a tendency to invade, there are very few reports on nonfunctioning NETs, especially omental NETs, excluding pancreatic and gastrointestinal. 9 Hence, treatment strategies for omental NETs, lack a consensus and may depend on the specific conditions and characteristics of each patient.
Similar to the approach adopted for nonfunctioning pancreatic NENs, we propose a resection policy whenever feasible, unless resection is excessively invasive. Minimally invasive surgery is recommended as the preferred procedure, with consideration for adjuvant therapy based on post-resection histopathologic findings. We believe that this approach aligns with the treatment of solitary nonfunctional NENs, such as omental NET.
In our case, NET was discovered incidentally. Intra-operative findings showed that the lesion was confined to the omentum and complete resection of the tumor alone was possible. As no other findings after systemic examinations suggested a primary lesion, omental NET was diagnosed. Given that the patient had non-functioning NET-G2, postoperative adjuvant chemotherapy for colorectal cancer was selected over that for NEN. Because the tumor was confined to the omentum and did not require adjuvant chemotherapy, future follow-up is important.
In a review of the literature, Terai reported the first omental NET in 2021. 9 According to this report, laparoscopic tumor resection for diagnostic treatment of NENs is reasonable and safe. This second case report for omental NET. Further case studies are required to obt-ain consent on the etiopathogenic mechanisms and its treatment.
Conclusion
We described a case of omental NET, which is extremely rare, with only 2 cases, nonfunctional NET. There is no consensus treatment strategy for it, and we hope to gather more cases in the future.
Footnotes
Acknowledgements
The authors would like to thank Dr. Nitta for his valuable guidance and insightful comments and Dr. Takeshita for their valuable insights and comments on the pathological analysis throughout the course of this research.
Author’s Note
The abstract of this study has been previously presented at the Japan Surgical Association, Okayama, Japan, November 18, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Ethics Committee of Medico Shunju Shiroyama Hospital.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.