
Abstract
Neuroendocrine tumors (NETs) are a heterogeneous group of tumors developing from neural crest cells, with numerous sites of origin, commonly the gastrointestinal and genitourinary tracts. NETs of the genitourinary tract are more common in women. Small cell carcinoma of the prostate or testicular carcinoid are the NETs in male. In this article, we present a rare case of NET of the scrotum. Our patient was a 47-year-old male with a history of complicated pilonidal cysts resulting in chronic scrotal wounds. Biopsy of a large nonhealing scrotal wound revealed a high-grade neuroendocrine carcinoma with features most suggestive of small cell carcinoma. Presenting with advanced disease at diagnosis, he was started on systemic therapy and unfortunately progressed through multiple lines of treatment, including CAPTEM (capecitabine and temozolomide). Unfortunately, due to multiple logistical reasons, the patient was unable to receive the then off-label immunotherapy based on DART (Dual Anti-CTLA-4 and Anti-PD-1 Blockade in Rare Tumors) trial. He, unfortunately, succumbed to his disease within months of diagnosis.
Introduction
Neuroendocrine tumors (NETs) are a heterogeneous group of relatively rare tumors, comprising ~2% of all malignancies, with a prevalence of <200 000 in the United States. They arise from neural crest cells and, hence, can have various sites of origin. 1 They are more commonly found in the lungs and gastrointestinal tract, but are rare in the genitourinary tract.2,3 They are more common in women. 3 Most male genital tract NETs are prostatic small cell carcinomas or testicular carcinoids. Small cell carcinoma is extremely rare in the scrotum, penis, and penile urethra. 3
NETs are divided into 2 groups based on clinical behavior, histology, and proliferation rate: well-differentiated (low grade to intermediate grade) and poorly differentiated (high grade) NETs. 2 We report a case of poorly differentiated NET of the scrotal skin with rapidly progressive clinical course at this rare site.
Case Presentation
The patient was a 47-year-old male with a complicated urological history due to recurrent pilonidal sinus requiring multiple perineal surgeries. It eventually led to the development of a fungating perineal wound and an urethro-cutaneous fistula, for which a urethroplasty was done. Perineal skin pathology obtained at the time of urethroplasty showed inflammation and fibrosis, but no evidence of malignancy. Two months post urethroplasty, the patient noted worsening scrotal swelling. A computed tomography scan of the pelvis with contrast revealed enlarged bilateral inguinal lymph nodes measuring 2.3 and 3.0 cm. Bilateral hydroceles were present, but there was no clear evidence of a discrete mass. He was managed conservatively with close follow-up. A few months later, he presented to the emergency department with painful and indurated swelling of the scrotum. Repeat computed tomography scan done at this time showed a mass measuring around 13 × 6.8 cm at the base of the penis with moderate bilateral pelvic and bilateral inguinal lymphadenopathy, consistent with metastatic disease (Figure 1).

Computed tomography pelvis with contrast showing bilateral pelvic and groin lymphadenopathy with penile base mass and scrotal edema.
This prompted an urological evaluation with surgical exploration. Extensive wound debridement was performed, and a biopsy of the scrotal mass obtained. The biopsy showed a poorly differentiated malignant neoplasm with extensive necrosis infiltrating adipose tissue. The tumor was composed of cohesive sheets of hyperchromatic cells with scant cytoplasm, nuclear molding, and dispersed chromatin (Figure 2A and B). Immunohistochemistry staining was positive for synaptophysin (Figure 2C), chromogranin (Figure 2D), and CAM5.2, but negative for CK7, CK20, CDX2, uroplakin II, GATA3, p63, and CK5/6. Additional immunostains showed the tumor cells to be positive for INSM1, while being negative for WT-1, desmin, CK7, and Merkel cell polyomavirus. Ki-67 showed a high labeling index of ~80%. This histopathology and immunophenotype profile supported the diagnosis of a high-grade NET, with features consistent with small cell carcinoma, arising from scrotal skin. Next-generation testing on the tumor sample revealed no targetable mutations, no microsatellite instability (low) and a tumor mutation burden (TMB) of 9. The histopathology was second reviewed at a high-volume center as well.
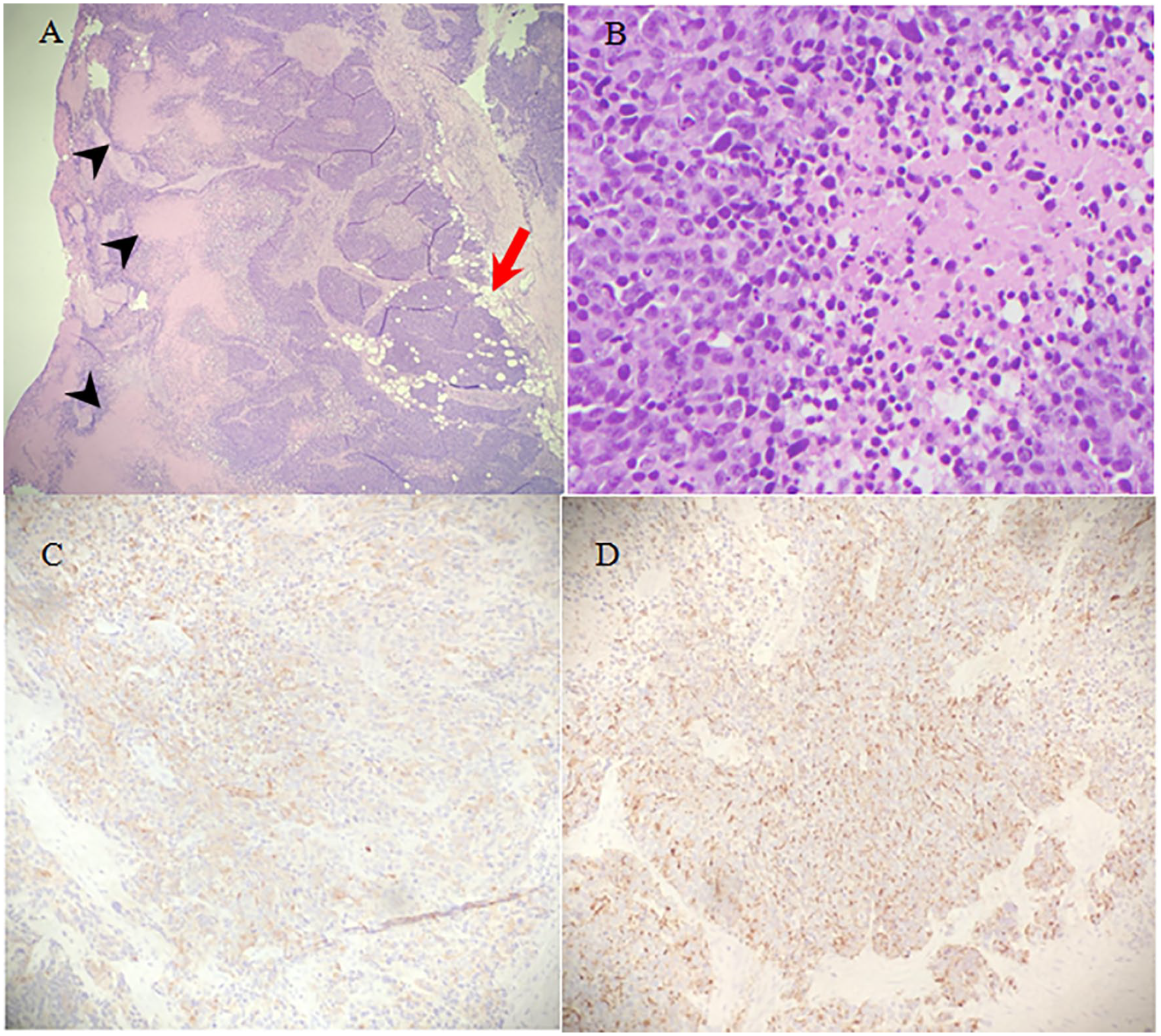
(A) Shows a malignant neoplasm with multiple areas of necrosis (black arrowheads) infiltrating adipose tissue (red arrow). (B) Shows poorly differentiated, hyperchromatic tumor cells with scant cytoplasm (left) adjacent to an area of necrosis (right). (C and D) demonstrate tumor cells staining positive for synaptophysin and chromogranin, respectively, consistent with a diagnosis of high-grade neuroendocrine carcinoma.
Chemotherapy has been the historical treatment of choice for high-grade NET. Hence, the patient was treated with 4 cycles of carboplatin and etoposide over a duration of 3 months. Unfortunately, restaging scans showed progression prompting a change in treatment to cisplatin and irinotecan, of which he received 3 cycles over 3 months. The patient’s treatment course was complicated by neutropenia; in the interim also showing disease progression, with worsening abdominal lymphadenopathy, this time with metastatic skin deposits for which he was offered palliative radiotherapy with weekly cisplatin over 2 weeks. Subsequent scans noted further progression in the scrotum, penis, and bulky retroperitoneal lymphadenopathy. Attempts to use immunotherapy were unsuccessful due to insurance issues as at that time, this was considered off-label. He was switched to third-line treatment with capecitabine and temozolomide (CAPTEM), around 7 months after his diagnosis, of which he was able to tolerate 2 cycles with continued rapid progression necessitating a hospitalization for symptom control. He was evaluated by the palliative care team and ultimately transitioned to hospice care, passing away within months after diagnosis.
Discussion
Scrotal carcinomas are a rare entity, occurring mostly as either basal cell or squamous cell histology. NETs of the scrotum are even rarer. NETs are a heterogeneous group of tumors, classified according to the originating site, histopathology proliferation index, and mitotic rate count. Extrapulmonary NETs are less common and are broadly classified into well-differentiated and poorly differentiated histological subtypes. Poorly differentiated subtypes confer a poor prognosis, characterized by a high mitotic index, high proliferation index, which rarely secrete amines or hormones and often present with local metastases. Our patient had an aggressive disease course, progressing through multiple lines of chemotherapy. Use of dual immune checkpoint blockade was considered based on the data from the DART trial, using ipilimumab and nivolumab, which revealed an overall response rate of 44% in patient with high-grade carcinoma (independent of tumor site), with one patient reaching an unconfirmed complete response. The 6-month progression-free survival was 31%, with a medial overall survival of 11 months among those with high-grade tumors. The proposed hypothesis was that high-grade neuroendocrine cancers could have a higher tumor mutational burden, allowing for a better response to immunotherapy. 4 Unfortunately, immunotherapy could not be used due to insurance issues.
We treated him with temozolamide and capecitabine, based on data from the CAPTEM studies done previously. CAPTEM have been known to be active in the first-line setting for advanced pancreatic neuroendocrine neoplasms. 3 A meta-analysis to study safety and efficacy of treating patients with advanced NETs with CAPTEM showed the combination to be both effective and relatively safe in a variety of different malignancies.5,6 In addition, the high objective response rates, achieved with CAPTEM makes it natural choice for patients who are heavily pretreated and “chemo resistant” until this regimen.5-7
A comparison of our case and cases published since 2019 has been summarized in Table 1.
A Summary Comparing Our Case to Cases Reported on Scrotal NETs Since 2019.

Abbreviations: MSI, microsatellite instability; N/A, not available; NETs, neuroendocrine tumors; TMB, tumor mutation burden.
Neuroendocrine carcinomas represent a heterogeneous tumor entity, with scrotal NETs being quite rare. Early diagnosis and treatment are of paramount importance, because of the aggressiveness of some tumor types.
Footnotes
Acknowledgements
Our sincere thanks to the Department of Hematology and Oncology at the Upstate University Hospital for all the support and guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Patient identifiers have been removed. Hence informed consent has not been obtained.