
Abstract
Tuberculosis (TB), caused by Mycobacterium tuberculosis, is a leading infectious disease with varied manifestations. We report a rare presentation of gastric TB in a 50-year-old immunocompetent woman from the Middle East with no prior medical history. The patient presented with persistent epigastric pain, weight loss, nausea, and vomiting over a 2-month duration. Imaging studies and an infectious disease panel were inconclusive. However, upper endoscopy revealed a subepithelial lesion at the pylorus, with biopsies demonstrating caseating granuloma and multinucleated giant cells. A QuantiFERON test was subsequently positive for TB. The patient was successfully treated with standard TB quadruple therapy, resulting in significant improvement in symptoms during follow-up. This case underscores the importance of considering extrapulmonary TB in immunocompetent patients with atypical gastrointestinal symptoms and highlights the efficacy of prompt antitubercular therapy.
Keywords
Introduction
Tuberculosis (TB) has historically caused more human fatalities than any other disease. Prior to the COVID-19 pandemic, TB was the most prevalent infectious disease. 1 The primary pathogen responsible for TB is Mycobacterium tuberculosis, an aerobic, non–spore-forming, and nonmotile bacterium. Upon inhalation, the M tuberculosis laden droplets can be eradicated, remain dormant (latent TB), or progress to active TB disease. The latent phase is characterized by granuloma formation, which are clusters of immune cells aimed at containing the bacteria and preventing its spread. 2 However, in immunocompromised adults with a CD4 count below 200, elderly patients, and children, these granulomas can deteriorate into pneumonia, leading to progressive active TB that can disseminate throughout the body.
Pulmonary TB is the most common manifestation of TB, typically presenting with chest x-ray abnormalities such as infiltrates, cavitation, and lymphadenopathy. 3 Extrapulmonary TB, accounting for about 15% of all TB cases, frequently affects the lymphatic system, central nervous system, musculoskeletal system, genitourinary tract, gastrointestinal tract, and peritoneum. 4 Gastrointestinal TB is rare, comprising only about 2% of TB cases, with the ileocecal region being the most common site. 5 The TB involving the stomach is exceptionally rare. This case report discusses an uncommon presentation of gastric TB in an immunocompetent patient.
Case Presentation
A 50-year-old woman who had no major medical history came to the Iraqi outpatient clinic complaining of abdominal pain for 3 months. The epigastric region was the site of intermittent, nonradiating pain that worsened after eating. Treatment with proton pump inhibitors provided no relief. The pain was accompanied by a 9-pound weight loss over a 2-month duration, along with nausea and 2 episodes of vomiting within a week. There were no associated symptoms of heartburn, melena, hematemesis, abdominal distention, or fever. Physical examination revealed mild epigastric tenderness, and her body mass index was 22.8 lb/in².
Laboratory findings revealed a hemoglobin level of 10.2 g/dL, a white blood cell count of 5900/µL, a platelet count of 280 000/µL, and an erythrocyte sedimentation rate of 11 mm/h. Liver function tests showed an alanine aminotransferase level of 29 U/L and an aspartate aminotransferase level of 38 U/L. The infectious disease panel was negative for anti-HCV Ag, HBsAg, anti-HBs, and HIV.
Diagnostic imaging, including chest x-ray and abdominal ultrasonography, revealed no abnormalities. Upper endoscopy revealed a lax cardia, thickened mucosa, and a poorly distensible, tube-like lumen at the cardia and body. It showed a polypoid-like lesion protruding from the pylorus toward the gastric antrum, suggestive of a subepithelial mass (Figure 1A). The endoscopy also demonstrates diffuse thickening of the gastric mucosa, leading to a narrowed and poorly distensible stomach with features resembling linitis plastica (Figure 1B). Initially, Crohn disease was considered a diagnosis, but this was later excluded based on biopsy findings and additional tests. The biopsy from the pyloric lesion revealed an ill-defined caseating granuloma, characterized by a central area of necrosis surrounded by aggregates of inflammatory cells, predominantly histiocytes, indicative of a chronic inflammatory process. No malignant cells were observed in the sample (Figure 2). Further diagnostic evaluations, including chest computed tomography and colonoscopy, did not reveal any additional pathological findings, which helped exclude Crohn disease. The QuantiFERON test was positive, serum angiotensin–converting enzyme levels were normal, and although the initial Mantoux test was negative, a repeat test showed progression with an induration measuring 12 mm.
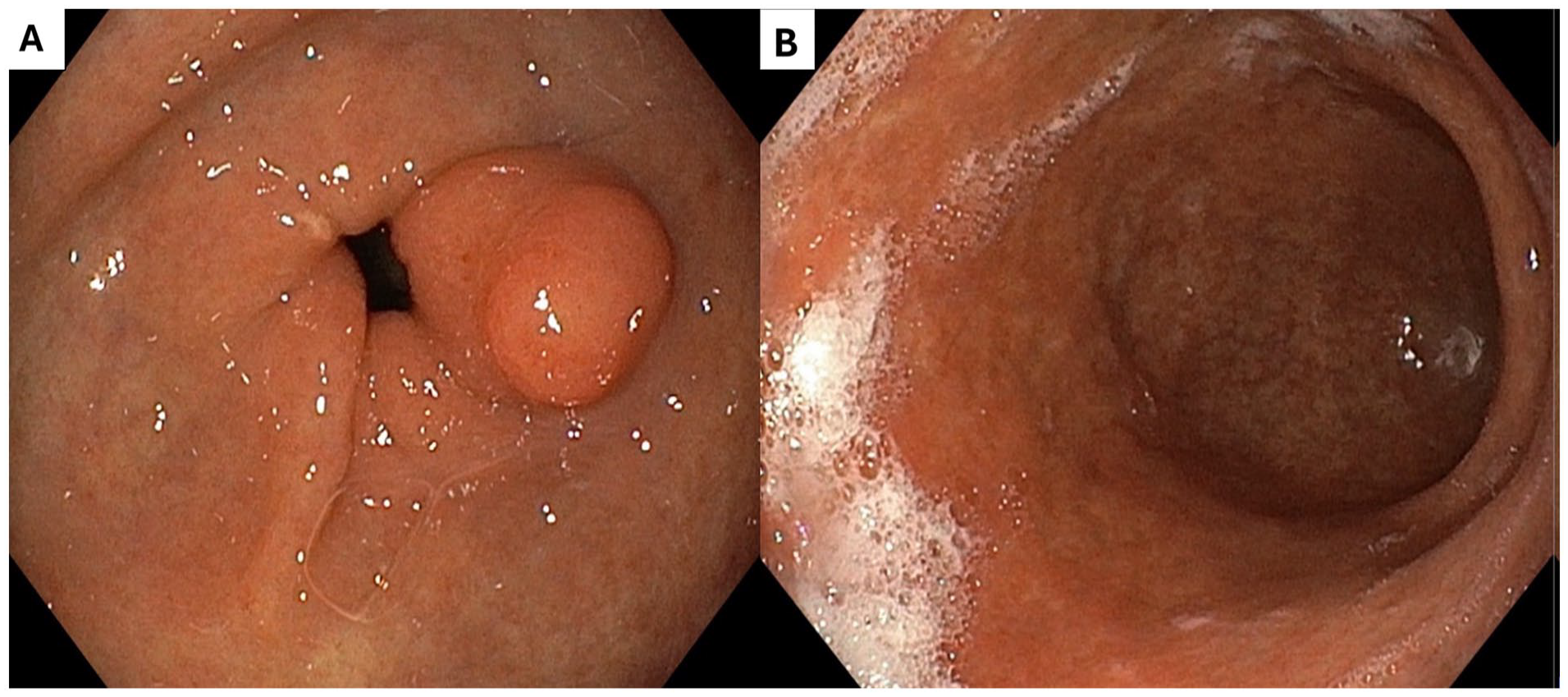
(A) shows a polypoid-like lesion protruding from the pylorus toward the gastric antrum, suggestive of a subepithelial mass, while (B) demonstrates diffuse thickening of the gastric mucosa, leading to a narrowed and poorly distensible stomach with features resembling linitis plastica.

(A) shows an ill-defined nodule with a caseating granuloma under low magnification, characterized by a central area of necrosis, surrounded by aggregates of inflammatory cells, predominantly histiocytes (macrophages), indicating a chronic inflammatory process, while (B) highlights the granuloma structure in greater detail, with high-power magnification of the inflammatory cells. No malignant cells are identified within the sample.
Based on these findings, we diagnosed TB and initiated treatment with standard TB quadruple therapy, consisting of rifampin, isoniazid, ethambutol, and pyrazinamide. The patient’s symptoms improved significantly within days. At a follow-up visit 3 months later, she had regained 5 pounds, and a repeat endoscopy demonstrated increased stomach distensibility and complete resolution of the gastric lesions.
Discussion
Despite extensive efforts in vaccination and chemotherapy, TB remains a leading cause of death from an infectious disease globally. 6 Our case involves an atypical presentation of TB in a non-immunocompromised individual, which is noteworthy given the rarity of gastric TB, constituting only a fraction of extrapulmonary cases.
Gastric TB is rare due to several protective factors of the stomach, including its high acidity, lack of lymphoid tissue, and the barrier function of the gastric mucosa. The patient’s presentation with persistent epigastric pain, weight loss, and vomiting without improvement on proton pump inhibitors prompted further investigation. The diagnostic challenge in this case was significant, given the nonspecific symptoms and the rarity of the disease’s gastric manifestation.
The literature suggests that TB can spread to the stomach through multiple pathways, including ingestion of infected sputum, hematogenous spread, or direct extension from adjacent infected lymph nodes. In our patient, the presence of a subepithelial lesion at the pylorus might have provided a breach for M tuberculosis to establish infection. This is supported by other findings where gastric TB typically presents with lesions in areas susceptible to mucosal breaches, such as the lesser curvature. 7 The diagnosis was ultimately confirmed through endoscopic biopsy, which is crucial as it allows for direct visualization and sampling of suspicious lesions. It underscores the importance of maintaining a high index of suspicion and pursuing aggressive diagnostic approaches in atypical cases.
Endoscopic findings in gastric TB can often mimic those of gastric cancer or peptic ulcer disease, with ulcers and hypertrophic masses commonly observed. 8 Studies have noted poor biopsy yields even in ulcerated lesions due to the failure of biopsy samples to include the submucosa, where TB granulomas reside. Polymerase chain reaction amplification of mycobacterial DNA may improve the rate of detection. However, false negatives are reported in 40% to 65% of cases. In addition, Maulahela et al. 9 reported that endoscopic ultrasonography is an excellent modality for characterizing TB lesions, as well as obtaining a sample for cytological confirmation of the diagnosis. This can aid in differentiating TB from other gastric pathologies. In addition, despite the patient’s initial Mantoux test results, the progression to a 12-mm induration on repeat testing highlighted the need for vigilance in monitoring TB exposure, especially in endemic areas.
The treatment of gastric TB does not differ significantly from pulmonary TB, involving a combination of isoniazid, rifampin, pyrazinamide, and ethambutol. This regimen proved effective in our patient, who showed significant symptomatic improvement and resolution of the pyloric lesion on follow-up endoscopy. 10 The case illustrates the critical nature of early and appropriate antitubercular therapy, which can lead to excellent outcomes even in cases of rare extrapulmonary manifestations.
Conclusion
This case highlights several important aspects: the necessity for high clinical suspicion of extrapulmonary TB in immunocompetent patients presenting with atypical abdominal symptoms in TB-endemic areas, the challenges associated with diagnosing gastric TB, and the effectiveness of standard TB treatment protocols in resolving rare manifestations of the disease. It serves as a reminder of the ongoing relevance of TB in global health and underscores the need for increased awareness and prompt investigation in cases with unusual presentations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.