
Abstract
Pulmonary embolism (PE) poses a significant health risk in the United States, with high mortality rates. Clinicians maintain a low threshold for suspecting PE, potentially leading to deviation from guideline-recommended algorithms and unnecessary computed tomography pulmonary angiography (CTPA). This case discusses a 46-year-old woman who presented with symptoms suggestive of PE following a prolonged road trip. Despite a low Wells score and negative D-dimer results, she underwent CTPA, resulting in an unnecessary and harmful interventional radiology–guided thrombectomy. This highlights the importance of adhering to guidelines in PE diagnosis to mitigate potential harms associated with the overuse of available medical tools.
Introduction
Pulmonary embolism (PE) is a serious health issue in the United States, with an estimated annual incidence of 39 to 115 cases/100 000 population. It causes more than 100 000 deaths annually, with a 30% mortality rate. Thus, clinicians must ensure prompt treatment of PE while remaining vigilant to avoid overdiagnosis. 1
Pulmonary embolism is considered a “great masquerader” among conditions, making its diagnosis challenging due to its diverse clinical presentations and ability to mimic other illnesses. Therefore, the possibility of overdiagnosing this grave illness can stem from cognitive biases shaped by the severity of the disease, the significance of early intervention, and mortality statistics. 2
In this case, despite a low Wells score and negative D-dimer, a patient with symptoms suggestive of PE underwent computed tomography pulmonary angiography (CTPA) leading to unnecessary and potentially harmful interventional radiology (IR)-guided thrombectomy, which was later found to be broncholithiasis. We present this case to stress the importance of following established diagnostic guidelines for PE, aiming to prevent unnecessary interventions while improving patient outcomes.
Case Presentation
A 46-year-old woman, with a medical history only significant for histoplasmosis and a family history of provoked deep vein thrombosis (DVT), experienced shortness of breath, cough, chest pain, and bilateral leg discomfort while on a prolonged road trip. Notably, she neither smokes nor takes oral contraceptives. She presented to a nearby health care facility with a blood pressure of 148/92, a heart rate of 77 beats/min, a respiratory rate of 19 cycles/min, and an oxygen saturation of 94% on room air. Table 1 shows an analysis of her Wells score.
Wells Score Components and Criteria With Assigned Points.

Initial laboratory workup, including the D-dimer and troponin, was negative, and the electrocardiogram showed no ischemic changes or signs of right ventricular strain. Computed tomography pulmonary angiography revealed a probable near-complete occlusion of the right upper pulmonary artery, affecting all 3 segmental branches (Figure 1A), along with significant calcification in subcarinal and stations 10R and 11R lymph nodes, right lower lobe, and spleen. Heparin infusion was started due to a suspected PE.
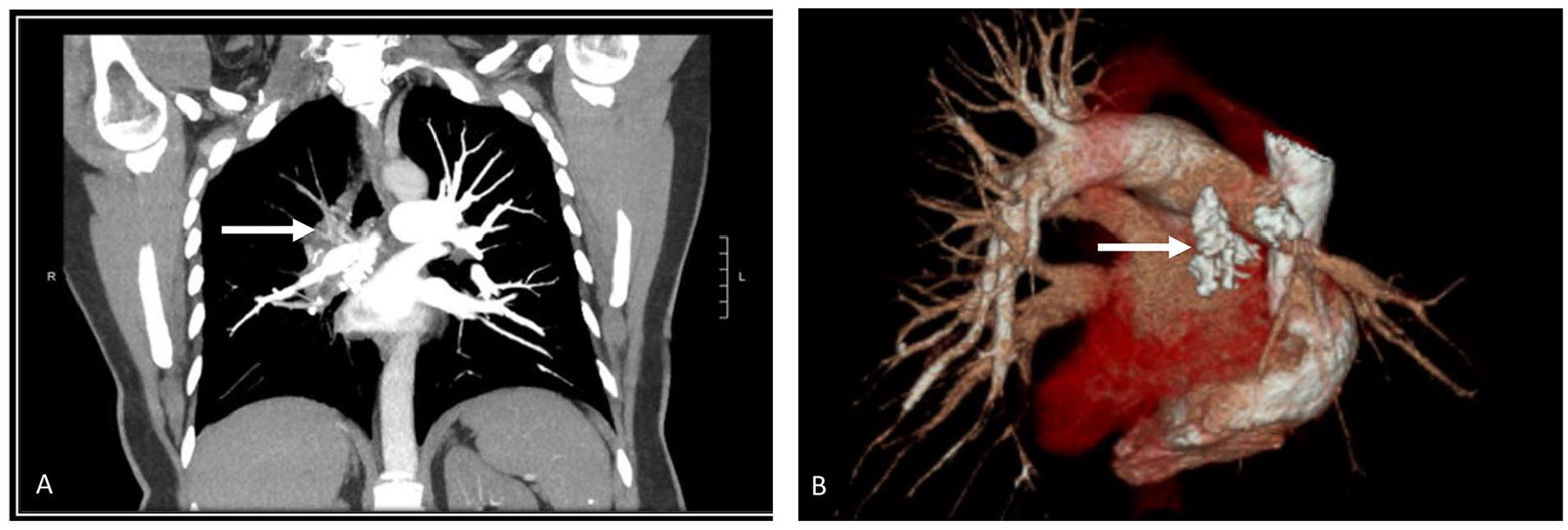
Lung-enhanced CT and 3D reconstruction revealed probable near-complete occlusion of the right upper pulmonary artery (A) and broncholith (Arrow) casing external compression of the right pulmonary vasculature (B)
The patient was transferred to our facility for the possible need for a thrombectomy to avoid chronic thromboembolic pulmonary hypertension. Interventional radiology–guided thrombectomy was attempted upon presentation, but no clot was found, and the procedure was eventually aborted due to the patient developing hypoxia and hemoptysis. Protamine sulfate was given to reverse the heparin effect. She was transferred to the intensive care unit (ICU) for monitoring. Further workup ruled out DVT on venous Doppler ultrasound of both lower extremities. Upon careful review of the computed tomography (CT) of the chest by the multidisciplinary team (Figure 1B), a broncholith abutting the wall of the right main bronchus was found, consistent with a diagnosis of broncholithiasis. This explained that the filling defect found in the right main upper pulmonary artery was due to external compression from the broncholith. Further investigations confirmed positive histoplasmosis antibodies. Her hypoxia and hemoptysis resolved, and she was safely discharged home.
Discussion
Patients with PE display diverse symptoms that resemble other diseases. Thus, clinical prediction tools like the Wells score and revised Geneva score are used to determine the likelihood of PE before further tests are conducted. 3 Guidelines suggest D-dimer testing if this evaluation yields a low or moderate probability and in cases where both the pretest probability and D-dimer results indicate a need for further evaluation, CTPA may be recommended. 3
When ruling out acute PE, D-dimer has a high negative predictive value. 1 The quantitative enzyme-linked immunosorbent assay has a minimum sensitivity of 95% and can rule out PE in patients with low to intermediate pretest probability. 1
A study conducted from 2016 to 2019 at 27 emergency rooms in the United States found that 5.3% of (1 828 010) patient encounters had PE diagnostic tests performed. A total of 25 870 patients had CTPA ordered without D-dimer (59% of all PE tests). From CTPA scans, the PE yield rate was 3.1%, which was positively linked with increased D-dimer ordering. Remarkably, women below 45 accounted for 21% of CTPA scans, and children made up 1.4%. 4 In another recent single-center study from Michigan, PE imaging yielded less than 2%, including 8449 patients over 2 years. According to Wells’ score, 96% of these patients had a low probability of PE. Just 37% of these patients with a low PE probability had D-dimer testing done. Unexpectedly, despite low Wells score and normal D-dimer levels, 260 patients underwent CTPA, yet none were diagnosed with PE. 5
The statistics from the mentioned studies provide valuable insights into the utilization and outcomes of PE diagnostic tests in health care facilities. The high percentage (59%) of CTPA scans ordered without D-dimer testing and the low yield rate, as low as 0% to 3.1%, suggest potential overutilization of imaging studies among multiple health care centers, highlighting the need for more targeted and evidence-based diagnostic approaches. This emphasizes that CTPA is not the first test to be performed in patients with suspected PE in every patient unless guidelines dictate that. This will result in minimizing unnecessary testing. In addition, the observed relatively high percentage of females who underwent CT images increases their risk of breast cancer, as will be mentioned later.
The advanced imaging capabilities of CTPA allow for identifying filling defects in subsegmental arteries as tiny as 2 to 3 mm in diameter. However, it is worth noting that some small clots may not require treatment, leading to a potential issue of overdiagnosis when detected. 6 Overdiagnosis of PE leads to unnecessary anticoagulation with harmful consequences. Anticoagulants carried a 5.3% risk of major bleeding in a large study, while the risk of recurrent venous thromboembolism was 0.7%. Furthermore, complications from anticoagulation for US hospitalized patients with PE increased from 3.1 to 5.3 per 100 000 between 1998 and 2006. 7
Computed tomography pulmonary angiography may lead to 3 cases of cancer per 1000 20-year-old women due to radiation exposure. 8 In addition, approximately 25% of CTPA find incidental lung nodules, thyroid nodules, or adenopathy, leading to further cancer evaluations, though most turn out to be false alarms. 6 Moreover, overdiagnosis causes patients harm due to inconvenience, anxiety, and increased health care costs. US hospital admission charges for PE surged from $25 000 to $44 000 between 1998 and 2006, excluding anticoagulation costs. 6
Guidelines and the Choosing Wisely Campaign have recommended that patients with a Wells score <4 and normal D-dimer do not require imaging. 6 Our patient’s Wells score of 3 placed her in the low-risk group, and with a negative D-Dimer, the CTPA could have been avoided. Unfortunately, overlooking these steps resulted in unnecessary interventions, including hospitalization, ICU admission, radiation exposure, invasive procedures, and ongoing anxiety. Following the guidelines for suspected PE is crucial to prevent such expensive, inefficient, and detrimental outcomes.
Conclusion
This case highlights the dangers of deviating from established guidelines in PE diagnosis. Overreliance on CTPA without proper risk stratification can lead to unnecessary interventions and increased health care costs, and potential adverse outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.