
Abstract
Half of the cases of pulmonary thromboembolism (PTE) are not diagnosed because of its unspecific clinical presentation; in Mexico, autopsy data reveal a similar incidence to that of developed countries. The objective of this work was to know the concordance between the clinical diagnosis of PTE at hospital discharge and its autopsy diagnosis. The method used was a retrospective cohort study of cases with PTE diagnosis who attended from January 2005 to December 2013. Information was obtained from the autopsies registry and clinical charts. From 177,368 hospital discharges, there were 412 (6.74%) with PTE diagnosis. There were 13,559 deaths, with PTE diagnosis in 139 (1%) patients. There were 479 autopsies, and in 66 (14%) of whom PTE diagnosis was documented, the mean age was 55 years (range, 18–89 years). The premortem diagnosis of PTE at discharge was confirmed in 412 cases. Postmortem diagnosis of principal disease was medical in 49 (74%) and medical-surgical in 17 (26%) patients. We found that nine patients had the clinical diagnosis of PTE, unlike the postmortem diagnosis, which was reported in 66 autopsies. The above allows establishing a 1:7 ratio that represents 14%. D-dimer was determined in 11 cases (16%) and was positive in 8 (73%). Thromboprophylaxis was applied in 15 cases (23%). The study of necropsies and identification of discrepancies is needed to improve the diagnostic accuracy and healthcare quality. The evaluation of hemostasis biomarkers besides D-dimer can better describe the pro-thrombotic state, the risk of thrombosis, and its association with morbidity and mortality.
Introduction
In the United States, there are 250,000 patients per year 1 diagnosed with pulmonary thromboembolism (PTE). The non-specific clinical presentation of PTE results in the diagnosis not being considered in up to 50% of patients, which underestimates its incidence. In most patients hospitalized with PTE, it is common to find a deep vein thrombosis (DVT). 2 In Europe, the incidence of PTE is 208/100,000 inhabitants per year. 3 In the United States, in hospitalized patients from 1979 to 1999, the prevalence of PTE was 0.4%. Mortality may reach 25% in patients who did not receive treatment, against 8% in those who received anticoagulant treatment, while fatal cases reached 11%. 4 The study conducted by Nordstrom and Lindblad 3 report 2356 autopsies, with an incidence of 595 cases with DVT (25%) and 431 (18.3%) with PTE; in 13% of the autopsies, PTE contributed to death. In hospitalized patients in the United States, the prevalence of PTE was 0.4%. 5 For massive PTE causes, mortality during the first hours of the event ranged from 65% to 95%; with the implementation of anticoagulant therapy, the mortality can be reduced to 75%, 6 although recurrence of DVT can reach 10% of patients with anticoagulant therapy. 7 Because of the high mortality rate and recurrence of DVT and PTE, it is considered a health problem that requires must opportune diagnosis and treatment.
In Mexico, an autopsy study indicates a concordance between all types of premortem and postmortem diagnoses of 40%. 8
The PTE, in most cases, is a consequence of DVT. The formation of a thrombus within a vein causes a partial or total occlusion that frequently resolves through endogenous fibrinolysis; if this does not occur, a clot forms in the venous system of the lower limbs and pelvis. 2 A venous thrombus may embolize to different arterial systems; the most frequently affected is the pulmonary system. 9
The frequency of predisposing factors in PTE patients may reach 80%.10,11 The concurrence of DVT and PTE becomes 90%; the origin of thrombi in the lower extremities occurs in approximately 50% of patients. 10 Asymptomatic PTE occurs during the postoperative period in patients who do not receive thromboembolism prophylaxis. 10 The PTE usually appears between the third and seventh day after DVT. It can be fatal from the first hour after the onset of symptoms. The resolution of PTE with the recovery of pulmonary perfusion may reach 60% of patients. The concept of a hypercoagulable state in patients with cancer is widely accepted. 12
The purpose of this work was to know the concordance between the clinical diagnosis of hospital discharge from PTE and the final diagnosis of the pathological study.
Methods
Study population
Sample size
Samples size was obtained from registered hospital discharges and necropsies recorded in the period from January 2005 to December 2013. No sample size calculation was made.
Inclusion criteria
(a) Cases registered with a diagnosis of PTE at the time of hospital discharge, or (b) autopsy records with a diagnosis of PTE from January 2005 to December 2013.
Exclusion criteria
Those cases with incomplete information were excluded.
Elimination criteria
Those files with non-identifiable pathological specimen were eliminated.
Study site
Hospitalary Unit of High Specialty level, Unidad Médica de Alta Especialidad, Hospital de Especialidades, Centro Médico Nacional de Occidente, Instituto Mexicano del Seguro Social, Guadalajara, Jalisco, México.
Type of study
A retrospective cohort design was conducted.
Data processing
Data processing was done by filling a database with the information obtained from (a) the official hospital discharge sheet, (b) the autopsy, and (c) clinical records (source document). The statistical analysis of data was supported by GraphPadPrism® software.
Statistical aspects
Descriptive statistics for numerical variables were supported using mean or median and standard deviation or minimum to maximum values as central tendency and dispersion measurements, depending on the parametric distribution or not. The proportions and percentages described the nominal or categorical variables.
Ethical considerations
The ethical considerations followed the Regulation’s general principles established by the General Law of Health Research (Ministry of Health).
Ethical approval for this study was authorized by Local Committee 1301 of Research and Ethics related to Research in the High Specialty Medical Unit of the Specialty Hospital, IMSS (R-2015-1301-121).
Informed consent was not sought for this retrospective study because it was considered as a minimum risk investigation, with confidential management of the information retrieved from clinical charts.
Results
From 2005 to 2013, there were 177,368 hospital discharges, of which 412 (6.74%) had PTE diagnosis (Table 1). In the hospital discharge flow of patients, there were 13,559 deaths, of which 139 (1%) was due to PTE (Table 2). The distribution and frequency per year are shown in Table 3.
Hospital discharge flow of patients with a diagnosis of PTE 2005–2013.

Dx: diagnosis; PTE: pulmonary thromboembolism.
Autopsy frequency and diagnosis of PTE, verified in the clinical diagnosis of the discharge registry from 2005 to 2013.
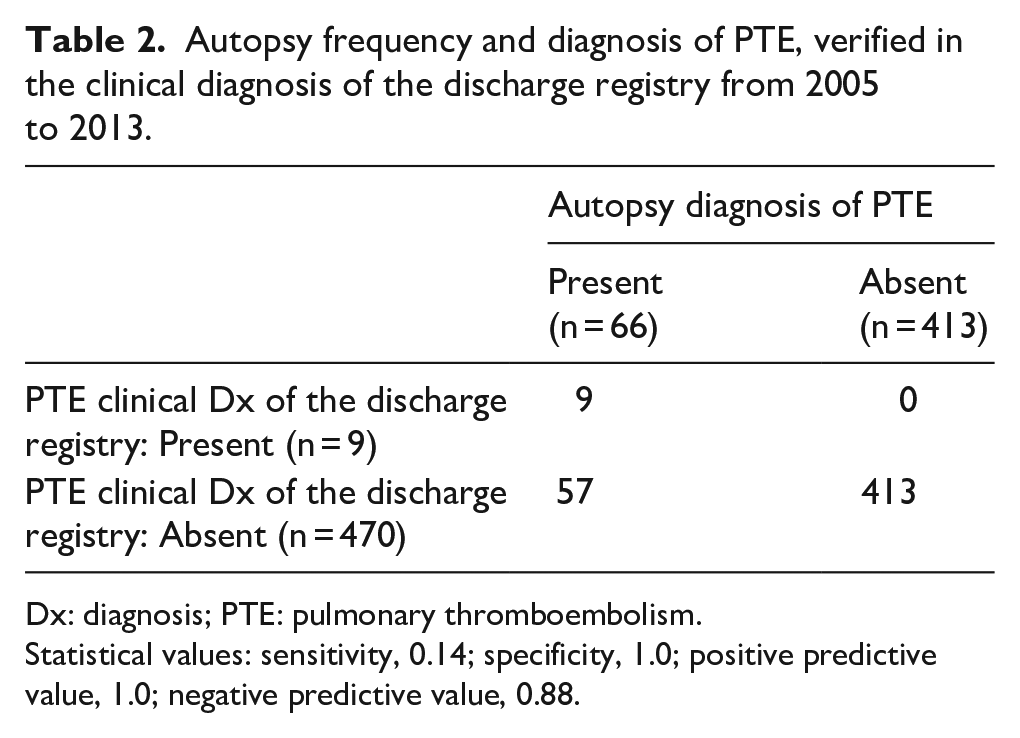
Dx: diagnosis; PTE: pulmonary thromboembolism.
Statistical values: sensitivity, 0.14; specificity, 1.0; positive predictive value, 1.0; negative predictive value, 0.88.
Frequency of PTE diagnosis at total hospital discharges and at total deaths during the period 2005–2013.

PTE: pulmonary thromboembolism.
The demographic data, clinical findings, and determination of D-dimer are shown in Table 4.
Clinical features of 66 cases with postmortem diagnosis of PTE.

PTE: pulmonary thromboembolism.
During the period of study, 479 autopsies were performed, of which 9 had a clinical diagnosis of PTE (which corresponds to 1.9% (7 women and 2 men)). A total of 66 autopsies had an anatomopathological diagnosis of PTE, 14% (35 females and 31 males), with an average age of 55 years (18–89, minimum–maximum). This group has a history of previous thrombosis in seven cases (11%).
The complementary clinical information was diagnosis of PTE before death in nine patients (14%) and the postmortem diagnosis in these cases in concordance with the final pathological diagnosis of PTE. The cause of death was PTE in 27 (41%) and associated disease in 29 (44%) patients, high concentration of D-dimer in 11 (17%) patients, and receiving thromboprophylaxis treatment in 13 (20%) patients—nine standard heparin and four low-molecular-weight heparin.
The summary of the hospital clinical diagnoses is shown in Table 5: respiratory diseases in 16 (24%) and cardiovascular diseases and cancer in 11 (17%), respectively; in two patients with cancer, the D-dimer concentration was determined to be elevated. Infectious diseases were found in 10 (15%), and the surgical procedure was found to be associated in 19 (29%) patients.
Frequency of diseases of 66 cases with postmortem diagnosis of pulmonary thromboembolism.

Discussion
In this study, we found a report of PTE in a total of 551 (0.31%) hospitalized patients, and 139 (1%) died due to acute PTE from the total deaths analyzed during the period. There were a total of 13,959 deaths, of which autopsy was performed only in 479 (3.43%) patients; the percentage variation per year was 2.5%–4.0% in the evaluated period; this result reveals a low percentage compared to other studies. 13
Tadlock et al. 14 reported that in 9 years they found PTE in 500 autopsies, and once five amniotic embolisms, three air, and one fat were excluded, they finalized with 491 venous thromboembolism.
In the hospital discharge report, nine patients had clinical diagnosis of PTE, unlike the postmortem diagnosis, which was reported in 66 autopsies. The above allows establishing a 1:7 ratio that represents a 14% agreement. Previously reported by Ornelas-Aguirre et al., 8 in this unit, a concordance of 40% was found between all premortem and postmortem diagnoses; in this study, the highest concordance of 76% was found in the diagnoses of cancer and obstetrics. Moreover, there was a low agreement of 5% of the diagnosis of respiratory diseases, without specifying the cases of PTE. 8
In a report including patients treated in an intensive care unit (ICU) for 25 years, 866 autopsies were performed in 2827 patients who died, corresponding to 30.3%. 15 They calculated the Class I errors with Goldman L. classification 15 in 63 (7.5%) patients, and 95 (11.4%) had type II errors, representing a potential impact on the therapeutic decision. The discrepancy was found mainly concerning PTE, pneumonia, and peritonitis, among others. This information points out the importance of performing clinical surveillance, the determination of biomarkers of hypercoagulation status, and the establishment of antithrombotic therapy.15,16
Currently, it is acceptable to perform laboratory tests to evaluate coagulation. Implementing this action will allow identifying on time the potential procoagulant state of patients at risk of thromboembolism, as are those patients with medical-surgical severe diseases. 17
Limitations of this study follow. As it is a retrospective study, it is appropriate to point out the bias in the enrollment of cases upon discharge from hospitalization and the clinical cases registry of the pathology department. Neither sample size calculation nor power calculation was made. We included consecutive cases from the described period January 2005 to December 2013.
In addition, there may be information bias as it has been collected retrospectively from the clinical record.
Conclusion
In this report, the frequency of PTE diagnosis in the whole group of hospital discharge was 0.31%, and 1% of deaths has a PTE diagnosis at hospital discharge.
Autopsies were performed in 479 patients, the previous consideration of the clinical diagnosis of PTE, of which 9 had a clinical diagnosis of PTE, which corresponds to 1.9% at the time of hospital discharge.
As relevant data, once the autopsy procedures were completed, the anatomopathological diagnosis of PTE reached 14%.
The study of necropsies and identification of discrepancies is necessary to improve the diagnostic accuracy, quality, and safety of health services.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was authorized by Local Committee 1301 of Research and Ethics related to Research in the High Specialty Medical Unit of the Specialty Hospital, IMSS (R-2015-1301-121).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for this retrospective study because it was considered as a minimum risk investigation, with confidential management of the information retrieved from clinical charts.