
Abstract
Takotsubo syndrome (TTS) is a transient ventricular dysfunction with apical ballooning triggered by emotional and/or physical stress. A few risk factors have been observed in patients with recurrent TTS, for example, excessive sympathetic stimuli, medications, stress, and tumors. Clinical features can vary from chest pain to overt hemodynamic instability. Diagnosis requires both electrocardiographic features and invasive imaging such as angiography to rule out other causes of cardiomyopathy prior to diagnosis. In addition, renal infarcts presenting as a complication of TTS are relatively uncommon. In this case report, we discuss the case of a 61-year-old African American woman with a prior history of TTS being managed for abdominal pain who developed a recurrence of the TTS during the hospital course. Prompt diagnosis and management of the condition is crucial to improve outcomes especially in patients with thromboembolic phenomenon or hemodynamic instability. Further large-scale studies are warranted to determine outcomes of patients with recurrent Takotsubo cardiomyopathy with thromboembolic phenomenon.
Introduction
Takotsubo syndrome (TTS) is a transient ventricular dysfunction with apical ballooning triggered by emotional and/or physical stress. It presents similar to acute coronary syndrome without coronary obstruction. 1 Recurrent TTS (RTTS) occurs after complete recovery of wall motion abnormality related to a previous TTS event. The RTTS is relatively uncommon, with reported incidence ranging from 1% to 6%. 1 In the United States, TTS accounts for 0.02% of the hospitalizations. 2 A few risk factors have been associated with RTTS, including concomitant pheochromocytoma, psychological stress, and medications, including chemotherapy. 3 Clinical features range from chest pain to overt shock. 4 Diagnosis requires clinical, electrocardiographic, and echocardiographic features suggestive of the syndrome with pertinent history and coronary angiogram to rule out ischemic cardiomyopathy. 5 Timely diagnosis and management of the disease are crucial to favorable outcomes. 4 Renal infarcts are relatively uncommon. According to one study, 21% of the patients had thromboembolic incidence, of which less than 1% experienced acute renal infarction. 6 Here, we present a case report of a 61-year-old African American woman with a prior history of TTS being managed for abdominal pain who developed a recurrence of the TTS during the hospital course.
Case Report
A 61-year-old African American woman with a past medical history of hypertension, dyslipidemia, type II diabetes mellitus complicated by gastroparesis and neuropathy, bilateral pulmonary embolism, and recurrent Helicobacter pylori infection, presented with a 3-day history of sudden-onset abdominal pain associated with loose bowel movements, nausea, and vomiting that progressed to chest discomfort prompting her to go to the emergency department. Prior to this presentation, she had been diagnosed with Takotsubo cardiomyopathy about 2 years ago and was being treated with goal-directed medical therapy, specifically low-dose metoprolol and angiotensin-converting inhibitors; her left ventricular function and wall motion had improved with the therapy. She also had a left heart cardiac catheterization that revealed patent coronary arteries. Her surgical history was significant for thyroidectomy, total knee replacement, and hysterectomy. She had been a former smoker and quit smoking about 5 years ago.
In the emergency department, vitals revealed a blood pressure of 124/97 mm Hg, heart rate of 114 beats per minute, respiratory rate of 18 breaths per minute, and saturation of 100% on room air. Physical examination revealed mild abdominal distension and hepatomegaly. Initial lab investigations were significant for leukocytosis, hyperglycemia, and mild ketonemia in blood. The investigations have been elaborated in Table 1. BioFire respiratory viral panel test is positive for enterovirus-human-rhinovirus. Chest x-ray did not reveal any acute abnormalities. Her electrocardiogram (ECG) showed marked T-wave inversion in limb and precordial leads. Computed tomography (CT) scan of the abdomen revealed colonic diverticulosis. She was admitted to the floor and managed with intravenous fluids and antibiotics.
Table Showing Abnormal Blood Tests Trend.

LVEF, left ventricular ejection fraction.
However, she intermittently complained of chest pain. An ECG on the floor revealed new ST-T changes and elevated troponin levels (troponin-140). The changes observed in ECG are shown in Figure 1. An echocardiogram revealed concentric left ventricular hypertrophy, left ventricular ejection fraction 35%, and a left ventricular mural thrombus (Figure 2). The patient was started on aspirin 81 mg, atorvastatin 80 mg, lisinopril, and metoprolol succinate. She was also started on a heparin drip for anticoagulation and shifted for telemetry monitoring.
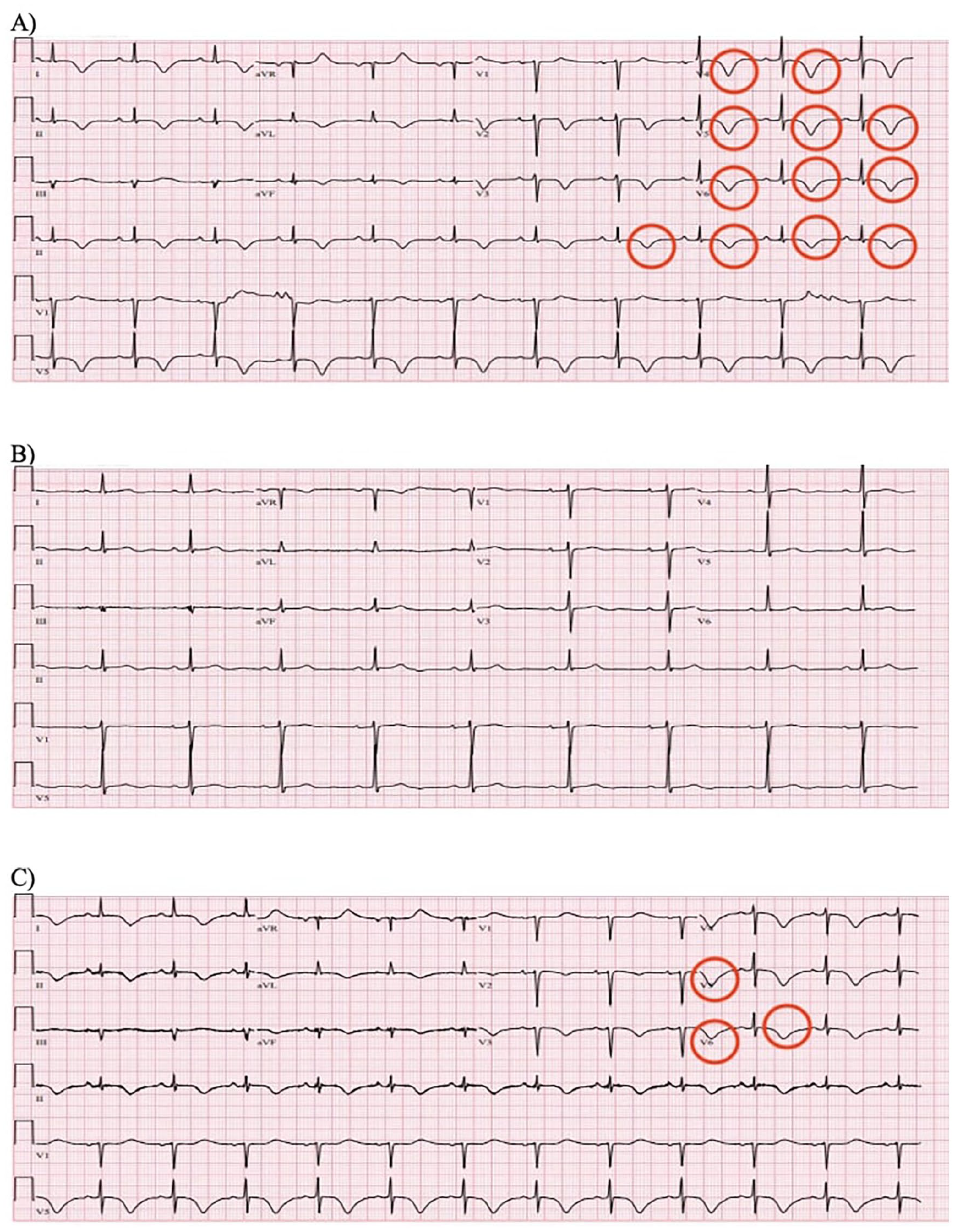
(A) Electrocardiogram (ECG) from 2021. (B) ECG from 2023 before presentation. (C) ECG from 2023 on presentation. In (A) and (C), we can see marked T-wave inversion in limb and precordial leads (circled in red).

Echocardiographic findings of the patient including left ventricular thrombus (circled in red).
However, the patient’s abdominal pain continued to persist. On day 3 of hospitalization, CT angiography of the abdomen revealed a large acute infarct of the left kidney with emboli in the hilar branches of the left renal artery, mild stenosis of the celiac trunk at the origin, large amount of noncalcified plaque projects into the aortic lumen, and pancolitis (Figure 3). She was then transferred to the intensive care unit for further management.

Computed tomography angiography of the abdomen revealed a large acute infarct of the left kidney with emboli in the hilar branches of the left renal artery, mild stenosis of the celiac trunk at the origin, large amount of noncalcified plaque projects into the aortic lumen and pancolitis (circled in red).
Vascular surgery and interventional radiology were consulted. No acute surgical interventions were recommended. The patient continued with a heparin drip. The gastroenterology team was also consulted for mild pancolitis and recommended to complete a 10-day course of oral ciprofloxacin and metronidazole and continue with oral esomeprazole. All the stool workup was normal.
The patient’s symptoms slightly improved, and she was transitioned to oral warfarin 4 mg once daily with a therapeutic international normalized ratio (2-3). She was discharged with an outpatient warfarin clinic appointment.
Discussion
The RTTS has been observed in middle-aged patients aged 50 to 70,5,7-10 as observed in our case. Interestingly, the disease has been observed in women mostly.4,5,7-13 The pathophysiology of recurrent Takotsubo cardiomyopathy has been linked with a postmenopausal estrogen decline consistent with the age spectrum of the patients.8,14 Estrogen is known to promote cardioprotective effects, including vasodilation and downregulation of β-adrenergic receptors. 14 In fact, female gender has been discussed as one of the predictors of recurrent Takotsubo cardiomyopathy. 15 A few risk factors have also been discussed in this regard, including factors predisposing to a catecholamine surge or rapid declination of the surge, for example, pheochromocytoma, thyrotoxicosis, opioid withdrawal, or hypoglycemia.4,9,14,16
Clinical features are relatively nonspecific and similar to features observed in acute coronary syndrome or heart failure exacerbation.5,7,8,9,10 In addition, symptoms can be completely unrelated to the underlying disease, as seen in a few cases.11,13 Electrocardiographic features commonly seen in TTS include strain patterns, multiple repolarization abnormalities, and T-wave inversions.5,7,9 The ST-segment elevation has also been described in a case from 2021. 17 In a few cases, changes might not be observed acutely.11-13 The ST-T changes are noted to result from underlying inflammation that can predispose to the development of TTS. 14
Echocardiographic features pathognomonic of TTS are akinesis of the basal segments or apex and left ventricular dysfunction.4,5,7-13 In a recent study, akinesis or ballooning of apical and midventricular segments is more likely to lead to the recurrence of TTS. 18 However, catheterization revealing patent coronaries is paramount for diagnosing TTS. 14
Management of the disease is based on 2 principles: optimization of therapy to treat cardiomyopathy and treatment to limit other cardiac risk factors. Beta-blockers are crucial in treating RTTS.5,8,11,13 Beta-blockers have been known to improve overall survival and decrease incidences of cardiogenic shock in patients with RTTS. 19 However, large-scale registries demonstrate that β-blockers might not significantly reduce the recurrence duration of TTS.19,20 Furthermore, comorbid conditions, such as anxiety, must be addressed.9,13
Complications associated with RTTS include left heart failure, mural thrombus and associated complications, cardiogenic shock, and ventricular arrhythmias. 14 A rapid turnover in microvascular dysfunction has been proposed as the mechanism for forming acute thrombus. In most cases, a quick lysis of the thrombus leads to resolution. However, a delay in lysis secondary to either coronary artery spasm or vasoconstriction can lead to an embolic phenomenon, as observed in our patient. 14 The embolic phenomenon has been described in one case with presenting features of ischemic enteritis, 21 but not renal infarction as observed in our case. It is suggested that embolic events in TTS may occur more frequently compared with acute myocardial infarction due to the improvement in the contraction of the apical myocardium, which could lead to the discharge of emboli from the apical thrombus. 22 A temporal relationship has been suggested in such cases with renal infarcts presenting within the first few days of development of thrombus and resolution of dysfunction. 22 Most of the patients usually require lifelong anticoagulation.7,11,12
Prognosis is usually favorable with low mortality rates except in a few cases,11,23 where the patients had presented with cardiogenic shock on admission, complicating the overall hospital course. Men generally have a worse prognosis. However, the incidence of Takotsubo cardiomyopathy in men is relatively less. 14
Conclusions
Recurrent Takotsubo cardiomyopathy is an uncommon phenomenon with microvascular dysfunction, vasospasm, and systolic dysfunction, further complicating the course of the disease. It is essential to diagnose the condition promptly to optimize management and outcomes, specifically in cases of cardiogenic shock or thromboembolism. Further large-scale studies are warranted to determine outcomes of patients with recurrent Takotsubo cardiomyopathy with thromboembolic henomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.