
Abstract
Mid-ventricular Takotsubo cardiomyopathy (TCM) is a variant of Takotsubo syndrome characterized by transient akinesis or dyskinesis of the mid-ventricular segments of the left ventricle, with sparing of the apical and basal segments. This differs from the typical apical form, which involves akinesis of the apical segments and hyperkinesis of the basal segments. Herein, we describe a unique case of mid-ventricular TCM presenting as cardiac asthma in a postmenopausal woman. Our patient reported a 2-day history of shortness of breath and intermittent wheezing that persisted even with respiratory treatment. Triage blood tests showed elevated troponin levels, and electrocardiogram was notable for septal Q waves, raising concern for acute coronary syndrome (ACS). Left heart catheterization revealed nonobstructive coronary artery disease, and ventriculography revealed mid-ventricular dyskinesia with a hypercontractile apex and base, consistent with mid-ventricular TCM. The ACS protocol was aborted, and the patient was managed conservatively with beta-blockers. Repeat echocardiogram at the 3-month follow-up showed recovered heart function, with no wall motion abnormalities.
Keywords
Introduction
Takotsubo cardiomyopathy (TCM), also known as stress-induced cardiomyopathy or broken heart syndrome, is a transient cardiac syndrome characterized by acute left ventricular dysfunction in the absence of obstructive coronary artery disease (CAD).1-4 While the classic apical ballooning variant is well recognized, atypical forms, including mid-ventricular variant, present unique diagnostic and clinical challenges. 2 The mid-ventricular variant of TCM is distinguished by hypokinesis or akinesis of the mid-left ventricle with preserved basal and apical contraction, often mimicking other cardiomyopathies or ischemic heart disease.2,5-8 Herein, we present a rare case of focal mid-ventricular TCM presenting as cardiac wheezing and dyspnea. Our patient presented with a 2-day history of shortness of breath and intermittent wheezing that did not improve with steroids and inhalers. Cardiac imaging confirmed mid-ventricular dysfunction with preserved apical contractility, highlighting the importance of recognizing this rare TCM subtype.
Case Summary
A 69-year-old woman with a medical history of hypertension and hyperlipidemia presented to the emergency department (ED) complaining of shortness of breath and intermittent wheezing for a few days. The patient was seen at an urgent center the day prior for similar complaints and was discharged with a short course of steroids and an albuterol rescue inhaler. She reported worsening of symptoms despite using the medications as recommended prompting the ED visit. She denied fever, chills, nausea, vomiting, acid reflux, acute dysphagia, cough, nasal discharge, chest pain, palpitations, extremity paresthesia, recent sick contact, or international travel. The patient was a lifetime nonsmoker and denied the use of alcohol and illicit substances.
In the ED, the patient appeared in no acute respiratory distress, with an oxygen saturation of 94% while breathing ambient air. The rest of the vital signs were normal. On examination, the patient had a symmetric chest rise, normal air entry bilaterally, and faint bilateral inspiratory and expiratory wheezing. There were no lung crackles, stridor, or stertor. The cardiovascular examination revealed a regular rate and rhythm, normal S1 and S2, and no murmurs, gallops or rubs. The remainder of the physical examination was unremarkable. Triage blood tests were significant only for troponin levels of 2675 pg/mL (normal range; 3-17). B-type natriuretic peptide, complete metabolic panel, complete blood count, and viral and bacterial pneumonia multiplex polymerase chain reactions panels were unremarkable.
The initial electrocardiogram (EKG) showed sinus rhythm with a ventricular rate of 75 beats per minute and septal Q waves. There were no over ST-segment deviations (Figure 1). The patient was admitted for acute non-ST-segment elevation myocardial infarction and treated with aspirin, clopidogrel, atorvastatin, metoprolol succinate, and weight-based enoxaparin. Although the chest X-ray showed no evidence of pulmonary disease, the patient was started on methylprednisone and albuterol-ipratropium, as needed, for suspected chronic obstructive pulmonary disease exacerbation. Computed tomography angiography of the chest was negative for pulmonary embolism, focal infiltrates, emphysematous changes, and pleural effusion. Transthoracic echocardiogram (TTE) revealed severely decreased left ventricular ejection fraction (LVEF; 20%-25%), impaired relaxation pattern of left ventricular diastolic filling, and moderately elevated pulmonary artery systolic pressure. The mid-inferoseptal, apical septal, apical, apical lateral, mid-anterolateral, apical anterior, apical inferior, and mid-anteroseptal walls were severely hypokinetic.

Electrocardiogram shows sinus rhythm with a ventricular rate of 75 beats per minute and septal Q waves (blue arrows).
Left heart catheterization (LHC) via the right femoral inguinal region showed nonobstructive CAD, and ventriculography revealed a LVEF of 35-40% with a hypercontractile apex and base (Figure 2). Mid-ventricular segment was dyskinetic, consistent with atypical TCM (Figure 3 and Supplemental Video 1). The patient tolerated the procedure well and hemostasis of the right common femoral artery was achieved using manual removal and pressure. Clopidogrel and enoxaparin were discontinued, and the patient was continued on aspirin, atorvastatin, and metoprolol succinate. On re-evaluation after the procedure, the patient denied any recent emotional stressors, illnesses, medical procedures, physical stress, or the use of stimulant beverages. An interval TTE at the 3-month follow-up showed a preserved LVEF and no wall motion abnormalities.

Coronary angiogram shows nonobstructive coronary artery disease.
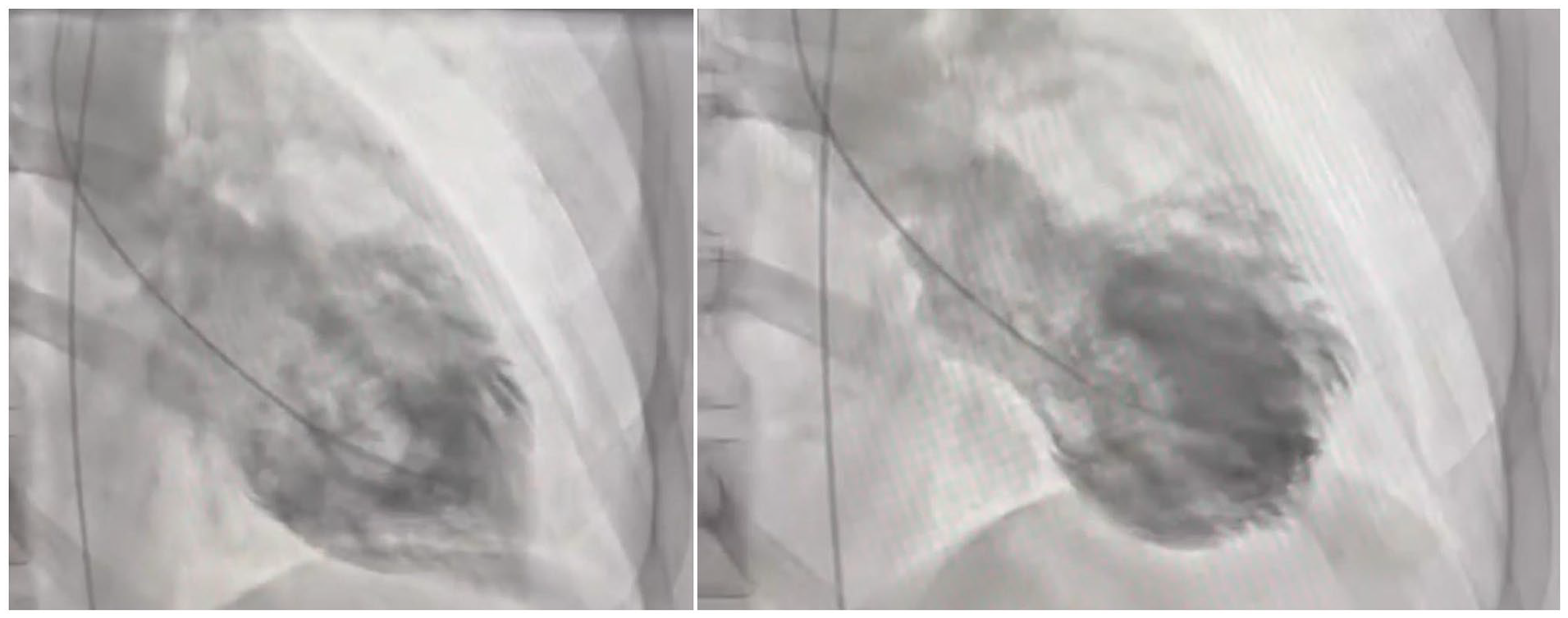
Left ventriculogram shows ejection fraction of 35% to 40% with hypercontractile apex and base. Mid-ventricular segment is dyskinetic, consistent with atypical Takotsubo cardiomyopathy.
Discussion
Mid-ventricular TCM is a variant of TCM characterized by transient akinesis or dyskinesis of the mid-ventricular segments of the left ventricle, with sparing of the apical and basal segments.1,9,10 This differs from the typical apical form, which involves akinesis of the apical segments with hyperkinesis of the basal segments. 1 Herein, we describe a unique case of mid-ventricular TCM presenting as cardiac asthma in a postmenopausal woman with no evident trigger. Our patient reported a 2-day history of shortness of breath and intermittent wheezing, which persisted even with respiratory treatment. Although there was an initial concern for acute coronary syndrome (ACS), LHC showed nonobstructive CAD, and ventriculography confirmed mid-ventricular TCM. The ACS protocol was aborted, and the patient was discharged with aspirin and atorvastatin for primary prevention of atherosclerotic cardiovascular disease. Repeat TTE at the 3-month follow-up showed recovered heart function, with no wall motion abnormalities.
First described in Japanese patients in the 1990s, TCM is a rare form of nonischemic cardiomyopathy characterized by acute left ventricular dysfunction due to an emotional or physical stressor.1,11 Common triggers include acute illness, emotional distress, major surgery, trauma, and substance withdrawal.1,12,13 Rarely, a joyous event can trigger TCM, a phenomenon known as “happy heart syndrome.”1,14,15 Patients with typical TCM are generally older (mean age ~67 years) and present with more pronounced left ventricular dysfunction and elevated BNP levels. 13 In contrast, atypical TCM variants including, mid-ventricular, basal, and focal, tend to affect younger patients. Cardiac imaging often shows higher LVEFs and lower or normal BNP levels on admission. 13 EKG findings also differ, with ST-segment depression more common in atypical cases, while ST-segment elevation is more frequent in typical cases. Atypical TCM forms constitute approximately 20% of all Takotsubo syndrome cases, with mid-ventricular variant being the most common subtype2,5,6,8 (Figure 4). Although our patient was older, the BNP level, EKG, and cardiac imaging findings were consistent with atypical TCM.

An illustration shows the different types of Takotsubo cardiomyopathy.
TCM etiopathogenesis remains unclear, largely contested, and it is thought to involve the brain–heart axis.1,11 Excess catecholamines, triggered by physical or emotional stress, contribute to myocardial injury through direct toxicity, oxidative stress, and calcium overload, leading to transient contractile dysfunction.1,2,7,11 Coronary microvascular dysfunction is also thought to impair myocardial perfusion further exacerbating regional wall motion abnormalities. 2 TCM and its variants typically present with chest pain, dyspnea, and diaphoresis, raising concern for ACS.2,6,11 Palpitations, syncope, fatigue, and weakness have also been reported in some cases. 6 Owing to its tendency to mimic ACS, the diagnostic workup for TCM often begins with troponin and BNP levels, thyroid-stimulating hormone, EKG, and echocardiogram. 2 EKG may show ST-segment deviations, T-wave inversions, QT prolongation, pathologic Q waves, or arrhythmias. 11 A fragmented QRS complex, low-voltage QRS complexes, and J wave have also been described.11,16 Our patient presented with elevated troponin level, normal BNP level, and septal Q waves. In the mid-ventricular subtype of atypical TCM, echocardiogram findings usually include transient left ventricular wall motion abnormalities, hypokinesis/akinesis of the mid-ventricle with preserved basal and apical contractility, and LVEF reduction, which typically recovers over days to weeks.2,11 Cardiac magnetic resonance imaging (MRI) can be obtained in uncertain cases, and it can differentiate TCM from ACS and myocarditis.3,4,7,14,17,18 Due to lack of fibrosis in TCM, cardiac MRI normally shows absence of late gadolinium enhance and myocardial edema in affected areas.2,11,19 Ioannou presented a unique case of iatrogenic adrenaline-induced mid-ventricular TCM in peripartum patient, which was diagnosed on cardiac MRI. 2 Invasive coronary angiogram helps distinguish TCM from ACS with no evidence of obstructive disease.
Once ACS has been ruled out, patients receive symptomatic care with oxygen for hypoxia, analgesics for chest pain, trigger-focused therapy.2,11 Hemodynamically stable patients are treated with beta-clockers to reduce adrenergic stimulation and prevent recurrence.1,11 Diuretics, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers may be considered in some cases to help with left ventricular function recovery and reduce overload.5,20 Unstable patients may require intravenous fluid resuscitation, vasopressors, and mechanical circulatory support with intra-aortic balloon pump or Impella in refractory cardiogenic shock. 11 Inotropes such as dobutamine and dopamine may worsen left ventricular outflow tract obstruction; therefore, they are typically avoided.11,20 Our patient was managed conservatively with beta-blockers to blunt the catecholamine surge, and interval echocardiogram showed myocardial recovery with no complications.
Conclusion
This case highlights the importance of recognizing mid-ventricular TCM as a rare but significant mimic of ACS and obstructive lung disease. Early identification and supportive management are crucial, as mid-ventricular TCM follows a generally favorable course with complete myocardial recovery. Further research is needed to better understand the pathophysiology and optimal management strategies of this atypical variant of TCM.
Footnotes
Author Roles
H.M. and L.B. conceptualized the idea of this case report. L.B., A.S., R.J., and J.R. assisted with data curation, literature review, and writing of the manuscript. S.E. and H.V. edited, fact-checked, and proofread the final version of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or cases series (<3 patients).
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability Statement
Further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.