
Abstract
Jehovah’s Witnesses is a Christian denomination widely recognized for their steadfast refusal of blood transfusions, even when facing severe anemia. We describe a unique case of a 42-year-old Jehovah’s Witness woman with severe iron deficiency anemia. She necessitated surgical correction of a malpositioned gastric band within the context of a complex necrotizing aspiration pneumonia secondary to esophageal obstruction. Medical management of this severe anemia has been a challenge as traditional approaches, like a blood transfusion, are not possible. Instead, a multifaceted approach has been described with intravenous iron infusions, recombinant human erythropoietin, vitamin B12, folate, and vitamin C administration. We emphasize the lack of consensus on guideline protocols regarding management of severe anemia for Jehovah’s Witness patients and the subsequent need for more investigation into that matter. It also underscores the significance of respecting patient autonomy through close collaboration between patients and their health care providers to ensure effective patient-centered care.
Introduction
Jehovah’s Witnesses is a Christian denomination widely recognized for their steadfast refusal of blood transfusions, even when facing severe anemia. Consequently, managing cases of critical anemia while adhering to their religious beliefs is challenging. Balancing the necessity to address a patient’s medical conditions with the imperative to uphold their religious autonomy can be intricate. This case report describes a patient who is a Jehovah’s Witness with severe iron deficiency anemia. She necessitated surgical correction of a malpositioned laparoscopic adjustable gastric band (LAGB) within the context of a complex necrotizing aspiration pneumonia secondary to esophageal obstruction.
Case Presentation
The patient is a 42-year-old Jehovah’s Witness woman with a past medical history of iron deficiency anemia, LAGB surgery 10 years prior, fibromyalgia, and schizophrenia. She presented with a 2-week history of progressive fever, shortness of breath, productive cough, postprandial solid vomitus, and chest pain. In the emergency department, she exhibited tachycardia and tachypnea. Her initial vital signs were as follows: blood pressure 122/76, pulse 132, temperature 98.6 °F, and respiratory rate 18. Physical examination revealed a nondistressed patient on 3 L of oxygen with decreased breath sounds present on the right lung compared with the left. There was dullness to percussion of the right upper and right middle lobes of the lung and significant crackles appreciated at the right middle lobe. Laboratory tests from her transfer hospital revealed marked leukocytosis at 33 TH/μL (reference range: 4-11 TH/μL) and microcytic hypochromic anemia with hemoglobin at 7.1 g/dL (reference range: 12.0-15.0 g/dL) (Table 1). A chest x-ray showed right lower lobe consolidation consistent with pneumonia. A computed tomographic (CT) scan of the chest revealed right lower lobe consolidation, a 4-cm right middle lobe abscess, a moderate to large loculated right pleural effusion, and marked diffuse distention of the esophagus, suggesting an aspiration etiology. Imaging indicated a malpositioned LAGB as the likely cause of esophageal obstruction (Figure 1). The LAGB was placed at an outside facility in 2010. She was seen by bariatric surgery in 2022 for chronic nausea and vomiting where it appeared her LAGB was malpositioned. At that visit, all fluid was removed from within the band port, and she was scheduled for a follow-up to discuss elective LAGB removal. Unfortunately, she was then lost to follow-up. The LAGB malpositioning more likely prevented the proper propulsion and digestion of foodstuffs the patient was ingesting, leading to the accumulation of foodstuffs in her upper gastrointestinal tract. This put her at an increased risk of aspiration and prevented the proper absorption of nutrients, including iron.
Laboratory Investigations.
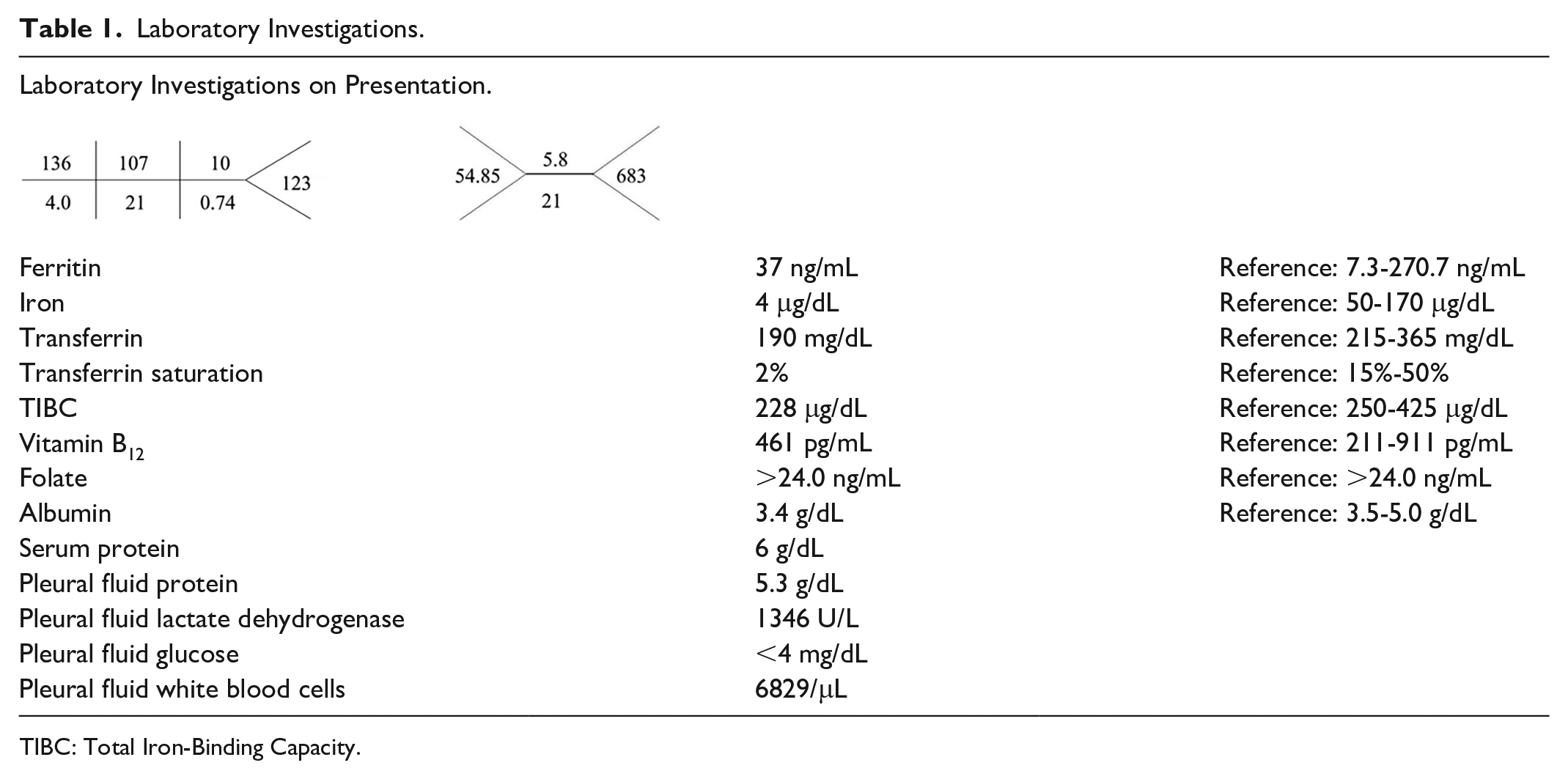
TIBC: Total Iron-Binding Capacity.

(A) The computed tomographic chest revealed diffuse distension of the esophagus with fluid up to the thoracic inlet level. (B) Distention of the lower esophagus and upper stomach with fluid proximal to the laparoscopic adjustable gastric band as evident in the topogram. (C) A sagittal section highlighting the distended esophagus. (D) Loculated pleural effusion (asterisk) and a right middle lobe abscess (arrow) are observed.
Prior to her hospital transfer to our facility, a chest tube was inserted, yielding over 2 L of greenish drainage. Pleural fluid analysis supported an exudative etiology (Table 1). Furthermore, the patient was initiated on intravenous ceftriaxone and metronidazole. She was kept strictly nothing by mouth due to esophageal obstruction caused by the malpositioned LAGB. Her fever, cough, and shortness of breath gradually improved. Surgical intervention was required to remove the malpositioned LAGB; however, her hemoglobin levels dropped to a nadir of 5.8 g/dL (reference range: 12.0-15.0 g/dL), and she adamantly declined blood transfusions. At this point, the patient was transferred to our facility for further evaluation by cardiothoracic surgery for possible surgical intervention on her necrotizing pneumonia and pleural empyema. Follow-up labs found that her iron was low at 4 μg/dL (reference range: 50-170 μg/dL), transferrin saturation low at 2% (reference range: 15%-50%) with a transferrin of 190 mg/dL (reference range: 215-365 mg/dL), and Total Iron-Binding Capacity (TIBC) of 228 μg/dL (reference range: 250-425 μg/dL). Interestingly, her ferritin was within normal limits at 37.0 ng/mL (reference range: 7.3-270.7 ng/mL), likely due to its role as an acute-phase reactant. Her vitamin B12 level, on the contrary, was within normal limits at 461 pg/mL (reference range: 211-911 pg/mL) and elevated folate of over our laboratory’s reference maximum of 24.0 ng/mL. Her albumin was found to be mildly deficient at 3.4 g/dL (reference range: 3.5-5.0 g/dL), but unfortunately pre-albumin was not drawn to assess her malnutrition status.
The patient was evaluated by cardiothoracic surgery on the day of transfer to our facility. At this time, surgical decortication was deferred due to her low hemoglobin levels and her marked leukocytosis. The patient’s intravenous ceftriaxone and metronidazole was continued, and she subsequently received 3 doses of intrapleural alteplase. Bariatric surgery was consulted on the day of transfer as well and anesthesia deferred LAGB removal as well due to the patient’s hemoglobin nadir and marked leukocytosis. Instead, her infection was continuously treated with antibiotics, and she was given supplements to increase her hemoglobin levels in preparation for surgical intervention. Prior to transfer to our facility, the patient received a 1000 mg course of intravenous iron sucrose and had a daily home dose of 325 mg of oral iron with questionable compliance. Within her hospitalization, the patient received repeat doses of 300 mg intravenous iron sucrose on hospital days 2, 4, and 6. Otherwise, she also received daily folic acid 1 mg, vitamin B12 1000 μg, and vitamin C 500 mg, in addition to 2 doses of erythropoietin (EPO) 10 000 units on hospital days 2 and 6. Phlebotomy was minimized by avoiding unnecessary blood draws and employing pedi-tubes for all necessary draws during her hospital stay, mitigating the risk of further hospital-acquired anemia. Her hemoglobin levels rose to 6.3 mg/dL on hospital day 5, and the general surgery team successfully removed the malpositioned LAGB without complication. Estimated blood loss during the procedure was minimal at 5 mL.
On postoperative day 4, after the removal of her LAGB and the day of discharge, the patient exhibited significant clinical and radiological improvement. Her hemoglobin was also measured to be 5.9 g/dL (Figure 2). However, she was found to be asymptomatic with her previous tachypnea resolved and with good blood-oxygen saturation on room air. On discharge, her antibiotic regimen was transitioned to oral amoxicillin/clavulanic acid for a total duration of 6 weeks. For continued management of her anemia, she was discharged on vitamin C 500 mg daily, vitamin B12 1000 μg daily, iron sulfate 325 mg every other day, and folic acid 1 mg daily. Continuity of these medications was left to be determined at the time of discharge and at the discretion of the patient’s primary care physician. Approximately 2 months after discharge, a repeat CT scan of her chest showed marked improvement in her cavitary consolidation in the right upper lobe and interval resolution of right pleural effusion, while her hemoglobin recovered impressively to 12.4 g/dL. At this time, her iron also recovered to 82 μg/dL with an appropriate transferrin saturation of 28% and ferritin of 36.2 ng/mL.

The patient’s hemoglobin values over her hospitalization. Her blood was drawn only on hospital days 1, 3, 5, and 9.
Discussion
The treatment of Jehovah’s Witness patients demands a multidisciplinary approach that respects their religious beliefs while delivering optimal medical care. Our patient presented with severe necrotizing aspiration pneumonia secondary to malpositioned LAGB. This challenge was accompanied by the presence of severe anemia. The medicine, general surgery, cardiothoracic, anesthesiology, gastroenterology, and pharmacology teams collaborated closely to plan the treatment course. After thoroughly explaining the potential risks and obtaining patient consent, the decision was made to proceed with surgery. However, managing the patient’s anemia without using blood transfusions in the setting of preoperative workup remained to be a challenge, due to limited guidelines for alternative interventions.
Although 7 g/dL is often observed as a standard threshold for transfusion, morbidity and mortality do not commonly increase until the hemoglobin drops below 5 g/dL in a patient. 1 This value can even be as low as 3 g/dL in patients without concurrent sepsis or trauma. 1 The combination of intravenous iron supplementation and recombinant human EPO has been a notable approach with documented success in literature for managing anemia among Jehovah’s Witness patients. 2 Some concerns were expressed regarding the safety of giving intravenous iron to this patient in the setting of severe infection, as iron supply is reported to promote pathogenic bacterial growth. 3 Interestingly, a systematic review and meta-analysis showed that intravenous iron therapy is not associated with an increased risk of infections, but severe infusion reactions were more common with intravenous iron. 4 Ultimately, the choice of using intravenous iron should be individualized to the patient’s condition. There is evidence that iron stores should be replenished in anemic patients for erythropoiesis-stimulating agents, which are used to stimulate red blood cell production, to be more effective. 5 Typically, in the setting of severe anemia, intravenous iron sucrose is given as a 100 mg intravenous push once daily for a total of 10 days. 6 There is conflicting evidence on the benefit of using EPO in a Jehovah’s Witness patient. Some literature demonstrates that treatment with low dose EPO was not associated with lower mortality. 7 However, administration of EPO in critically ill Jehovah’s Witness patients, such as experienced burns, general surgery, or gastrointestinal hemorrhage, was found to increase survival and hemoglobin levels. 8 Upon review of the literature, EPO is given as a dose of 40,000 units subcutaneously once every week with a hemoglobin >7 g/dL and as a dose of 20,000 units subcutaneously once a day for 5 days. 6 Of note, there are variations among Jehovah’s Witnesses regarding the acceptance of recombinant human EPO. In a retrospective review from 2015, 66% of Jehovah’s Witness patients accepted EPO. 9 Therefore, the decision to begin treatment with EPO and further treatment plan should be tailored to the patient’s personal beliefs and practices.
There are additional methods of intervention that are reported in literature that can be used to stimulate red blood cell production in conjunction with EPO, such as vitamin B12 and folate. 9 Vitamin B12 is given as a standard 1000 μg intramuscular injection once, while 1 mg folate is infused via intravenous piggyback once daily. 6 Vitamin K is also useful to activate the coagulation cascade through vitamin K–dependent coagulation factors, preventing bleeding and the further lowering of hemoglobin. There have been multiple reports of success using a similar combination of agents to those described above in Jehovah’s Witness patients with low hemoglobin levels.1,6,10
Vitamin C is another additional supplement that can increase non-heme iron absorption, along with evidence of directly inhibiting hepcidin expression which increases iron bioavailability. 11 Moreover, vitamin C was found to enhance erythropoietin receptor (EPOR) production, which may correct the downregulating EPOR from EPO, and this has additional effect with EPO in treating anemia. 12 However, there is conflicting evidence of the efficacy of vitamin C in treatment of iron deficiency anemia and its implementation should be considered in a comprehensive plan alongside other supplementation. 13
Nonmedical forms of intervention can also be used. Minimizing blood draws is important to prevent unnecessary blood loss in patients with critically low hemoglobin.
Commonly associated complications associated with LAGB include pouch enlargement, band slip, band erosion, port-site infections, and port breakage. 14 In this case report, the patient presented specifically with a type III band slip that involved a subsequent pouch enlargement. The most common etiology of this classification of band slips involves an overly tight band or overeating. These band slips are typically managed initially with conservative treatment like full band deflation and re-education on portion size control. 14 Our patient was initially managed with this conservative approach in 2022, but was subsequently lost to follow-up. Typically, this approach is successful in about 77% of patients and failure is defined as lack of resolution of pouch enlargement in an 8- to 10-week period on contrast imaging. 14 Given her infection and continual esophageal dilatation noted on imaging during her hospital stay, it can be concluded that our patient failed conservative management and required surgical removal of her LAGB.
We postulate that the patient’s underlying cause of her iron deficiency anemia was her malpositioned LAGB, resulting in an esophageal blockage and subsequent lack of absorption. Unfortunately, a pre-albumin was not drawn on our patient to assess the full extent of her malnutrition during her hospitalization. Her albumin, though, was only mildly low at 3.4 g/dL on admission (reference range: 3.5-5.0 g/dL) and dropped to a nadir of 2.5 g/dL on her date of discharge. In the literature, there is risk of bariatric surgery causing anemia, bone metabolism abnormalities, and protein malnutrition. 15 Iron deficiency is the most common cause of postbariatric surgery anemia, with vitamin B12 being second. 15 It is recommended that all patients receive screening for anemia prior to undergoing bariatric surgery. Unfortunately, there is not much research that has been done specifically evaluating the nutritional impacts of gastric band surgery. One study found a 41% decrease in folate levels in patients 24 months after gastric band surgery, whereas other studies have reported stability in folate levels.16,17 The long-term impacts on nutritional status in patients who undergo gastric band surgeries is an area of interest that should be further evaluated. While the malpositioning of the patient’s LAGB was a significant contribution to the severity of her anemia, it is important for physicians to be aware of the risk of anemia and other nutritional deficiencies in all bariatric surgery patients.
Conclusion
This case report describes the management of a Jehovah’s Witness patient with anemia declining blood transfusions in the setting of preoperative workup for an essential procedure. It describes multiple common treatment approaches that achieved some level of success in the literature; however, there is no consensus on guideline protocols and more research should be conducted in that matter, given the growing population of Jehovah’s Witnesses in the United States. Ultimately, patient autonomy is the most important factor in management, and all treatment methods should be discussed in-depth with patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MS4.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.