
Abstract
Achromobacter xylosoxidans is a gram-negative bacterium that is responsible for rare peritonitis associated with peritoneal dialysis (PD). We present a case of a 64-year-old woman with a medical history of end-stage renal disease undergoing PD who was admitted to the emergency department with abdominal pain and nausea. Physical examination and laboratory studies revealed peritoneal signs and laboratory abnormalities consistent with peritonitis. Intraperitoneal catheter dysfunction was identified and subsequently resolved via laparoscopy. Following a peritoneal fluid culture, A xylosoxidans was identified, leading to the initiation of intraperitoneal meropenem treatment. After an initial improvement, the patient developed an ileus and recurrent abdominal symptoms, and further peritoneal cultures remained positive for A xylosoxidans. Subsequent treatment included intravenous meropenem and vancomycin for Clostridium difficile colitis. Owing to the high likelihood of biofilm formation on the PD catheter by A xylosoxidans, the catheter was removed, and the patient transitioned to hemodialysis. Intravenous meropenem was continued for 2 weeks post-catheter removal. This case highlights the challenges in managing recurrent peritonitis in PD patients caused by multidrug-resistant A xylosoxidans. A high index of suspicion, appropriate microbiological identification, and targeted intraperitoneal and systemic antibiotic treatment, along with catheter management, are crucial in achieving a favorable outcome in such cases.
Introduction
Achromobacter xylosoxidans is a gram-negative bacterium that can cause infections in various clinical settings, including peritoneal dialysis (PD). 1 Immunocompromising status like malignancy and cystic fibrosis (CF) are the main risk factors. Peritoneal dialysis–associated peritonitis caused by A xylosoxidans is a rare but significant complication in patients undergoing PD. 2 Peritoneal dialysis–associated peritonitis has several complications, including prolonged hospitalization, 3 increased morbidity and mortality, and the need for catheter removal or transition to hemodialysis.4,5 Management of peritonitis caused by A xylosoxidans involves antibiotic therapy, which may require a combination of antibiotics, given the intrinsic resistance of the bacterium to certain antimicrobial agents. 6 The choice of antibiotics should be guided by susceptibility testing to ensure effective treatment. Antibiotic resistance is often reported during treatment of relapsed A xylosoxidans infections, and the antibiotic regimen is then updated to include antibiotics with greater sensitivity. 7 Most of the isolated strains exhibited susceptibility to empirical carbapenems and piperacillin/tazobactam in vitro, while resistance was observed against aminoglycosides, ciprofloxacin, ceftazidime, or trimethoprim/sulfamethoxazole, as reported in previous studies. 8 Antimicrobial resistance is a growing concern in health care settings, including PD units. The emergence of multidrug-resistant A xylosoxidans strains limits treatment options, leading to the requirement of alternative antibiotics or combination therapy.9-11 Close monitoring of antimicrobial susceptibility patterns and appropriate infection control measures are crucial for managing these infections and preventing the spread of resistant strains.12,13 In addition to antimicrobial resistance, other issues that arise during the treatment of peritonitis caused by A xylosoxidans include the need for catheter removal, risk of relapse or recurrence, and potential for complications such as peritoneal fibrosis or encapsulating peritoneal sclerosis.14,15 Therefore, early recognition, prompt treatment, and close monitoring of peritonitis episodes caused by A xylosoxidans are essential to minimize its negative impact on patient outcomes. 16
We present a case report of a patient with end-stage renal disease undergoing PD presenting with clinical manifestations of peritonitis.
Case Report
We report the case of a 64-year-old woman with a medical history of end-stage renal disease undergoing PD. The patient had been undergoing continuous cyclic peritoneal dialysis (CCPD) for 5 years. She was admitted to the emergency department after experiencing abdominal pain and nausea for 5 days. The abdominal pain gradually became severe and diffuse and worsened with PD treatment. The pain did not worsen during the filling and draining of PD fluids. She did not have emesis, fever, or chills and had no prior history of peritonitis. In addition, the PD fluid exhibited cloudiness.
Her vital signs on admission were as follows: blood pressure, 143/74 mm Hg; heart rate, 70 beats per minute; respiratory rate, 16 breaths per minute; oxygen saturation, 97% in ambient air; and temperature 97.4°F. Physical examination revealed a distended abdomen with tenderness during palpation across all 4 quadrants. Laboratory studies revealed the following: hemoglobin of 10.7 g/dL; white blood cell (WBC) count of 3.6 × 103 uL with 74% neutrophils; blood urea nitrogen of 52 mg/dL; creatinine of 8.32 mg/dL; and relatively normal electrolytes. Cell counts and cell cultures were performed on the peritoneal dialysate. Two liters of the dialysate were instilled, and only 1 L of cloudy fluid was drained after 2 hours. The cell count revealed 5138 WBCs, of which 60% were neutrophils. An attempt to flush the PD catheter yielded no fluid return even with aspiration. Intraperitoneal antibiotics were deferred because of catheter dysfunction, and the patient was administered empiric intravenous vancomycin 1 g every 5 days and cefepime 1 g every other day (Table 1).
Laboratory Parameters of the Case Reported.

General surgery service was consulted to evaluate the dysfunctional catheter. The patient underwent diagnostic laparoscopy, and the tip of the catheter was freed from a small obstructing adhesion, resolving the catheter dysfunction. The patient restarted continuous cyclic PD. The prescription was 5 exchanges of 2-L fills over 9 h, alternating 1.5% and 2.5% dextrose solutions; fill volumes of 500 mL were started and slowly increased to 2 L over several days postoperatively. On the fourth day after admission, the peritoneal fluid culture exhibited the presence of A xylosoxidans, which was susceptible to meropenem, piperacillin/tazobactam, and trimethoprim/sulfamethoxazole, resistant to amikacin, gentamicin, and tobramycin, and intermediately susceptible to cefepime and ciprofloxacin. AxyABM gene mutation was identified by polymerase chain reaction (PCR). The antibiotic regimen was changed from vancomycin/cefepime to intraperitoneal meropenem. Repeated cell counting and culturing showed that the peritoneal WBCs had increased to 8125, with 84% neutrophils. Subsequently, the patient experienced severe abdominal pain and constipation. Abdominal radiography revealed dilated loops in the small bowel related to the ileus. The patient was administered a bowel regimen of polyethylene glycol and psyllium husks, and her symptoms resolved. Treatment with meropenem was continued.
On day 8, the peritoneal WBC count decreased to 1256, with 87% neutrophils, and on day 10, the peritoneal WBC count was 0. The patient was discharged and completed a total of 3 weeks of intraperitoneal treatment with 1 g of meropenem daily. The peritoneal cell count upon the completion of antibiotic treatment showed 95 WBCs with 26% neutrophils; but the cultures remained negative. The patient again presented with nausea, abdominal pain, and 2 episodes of emesis and diarrhea 12 days after completing the antibiotic treatment. The patient had no fever or chills. The peritoneal cell count revealed 2513 WBCs with 93% neutrophils. The patient was administered intravenous meropenem 1 g daily and vancomycin 1 g every other day while awaiting culture results. The patient was also diagnosed with Clostridium difficile colitis based on a stool sample, for which she was treated with oral vancomycin 250 mg 4 times a day. Two days after the second admission, the peritoneal fluid culture exhibited the presence of A xylosoxidans with resistance patterns identical to those observed during the previous episode. Vancomycin was discontinued while intravenous meropenem was continued. On day 4, the patient underwent laparoscopic removal of the PD catheter to manage the relapsing peritonitis because of the high likelihood that the microbe had formed a biofilm on the PD catheter. The tip of the PD catheter also exhibited A xylosoxidans growth. The patient underwent a tunneled hemodialysis catheter placement the following day and was switched to hemodialysis. Intravenous meropenem was continued for 14 days after the removal of the PD catheter (Table 2).
Peritoneal Fluid Cell Count Overtime During Initial Hospitalization.
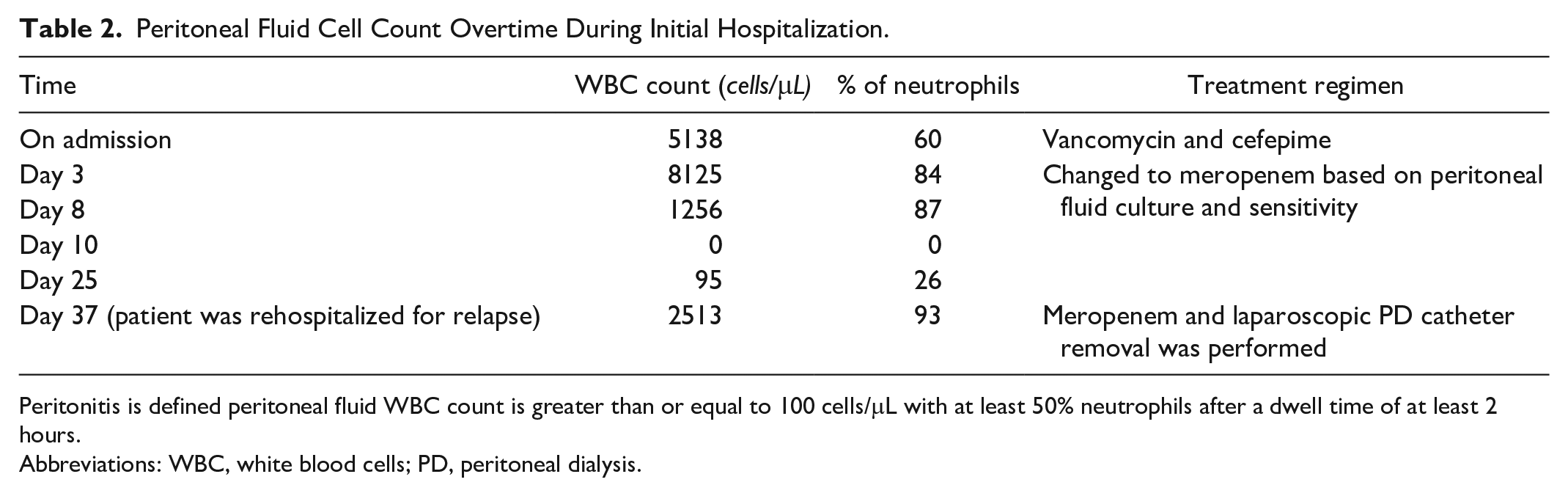
Peritonitis is defined peritoneal fluid WBC count is greater than or equal to 100 cells/μL with at least 50% neutrophils after a dwell time of at least 2 hours.
Abbreviations: WBC, white blood cells; PD, peritoneal dialysis.
Discussion
This case report describes the association of A xylosoxidans with PD-associated peritonitis and the subsequent relapse of the infection. In addition, we searched PubMed and Web of Sciences databases for relevant case reports, and reviewed articles published between 2010 and 2023. The following keywords were used for the literature search: A xylosoxidans, Peritonitis, PD, and Achromobacter infections. A xylosoxidans is known to exhibit resistance to various antibiotics, including quinolones, expanded-spectrum beta-lactams, aztreonam, and aminoglycosides. 17 The overproduction of AxyABM plays a role in the development of acquired resistance in Achromobacter against ciprofloxacin, meropenem, and ceftazidime. These antibiotics are commonly used in CF patients. Moreover, AxyABM overproduction also leads to an increase in the minimum inhibitory concentration (MIC) of the promising antibiotic cefiderocol. 18 In this case study, A xylosoxidans showed resistance to multiple antimicrobial agents, and meropenem was used for treatment. This was consistent with the observations in previous reports (Table 3). Studies have highlighted the challenges in treating peritonitis caused by A xylosoxidans, despite appropriate antibiotic therapy.2,19-24
Reports of Peritonitis Caused by Achromobacter xylosoxidans.

Abbreviations: IP, intraperitoneal; IV, intravenous; PD, peritoneal dialysis; NA, not applicable.
The selection of empiric antibiotics should consider the local antimicrobial susceptibility profiles. Monitoring antibiotic resistance among gram-negative bacteria, including A xylosoxidans, is crucial for the selection of effective antibiotic therapies. The virulence and high recurrence rate of peritonitis caused by A xylosoxidans, along with its resistance to commonly used antibiotics, may necessitate the removal of the PD catheter and a switch to hemodialysis. Biofilm formation, an intrinsic ability of many A xylosoxidans strains, contributes to its antimicrobial resistance and virulence, further complicating the treatment.2,19-24
In this case report, similar to that in previous reports, A xylosoxidans in PD-associated peritonitis exhibited resistance to multiple antibiotics, making treatment challenging. In our case, the culture confirmed the presence of A xylosoxidans resistant to multiple antibiotics, including beta lactams and aminoglycoside. There are 2 main mechanisms of intrinsic resistance of A xylosoxidans to multiple antibiotics. A chromosomal beta-lactamase like OXA-114, which can hydrolyze beta lactam antibiotics such as penicillin and cephalosporins, making them ineffective. The other mechanism is the development of efflux pumps by bacteria, such as AxyABM, AxyXY-OprZ, and AxyEF-OprN, which are proteins that transport antibiotics like aminoglycosides out of the cell, preventing them from reaching their target. 25
The selection of antibiotic regimens based on antibiotic susceptibility and resistance was supported by previous reports. Table 2 summarizes the presentation, treatment, and outcomes of the 7 prior cases reviewed. These prior cases have reported antibiotic resistance and biofilm formation by A xylosoxidans, similar to our findings. The PD catheter needed to be removed.
Conclusions
In summary, PD-associated peritonitis caused by A xylosoxidans is a rare but significant complication. It can lead to prolonged hospitalization, increased morbidity and mortality, and challenges in antimicrobial treatment owing to multidrug resistance. Management of A xylosoxidans infection requires appropriate antibiotic therapy guided by susceptibility testing and close monitoring of complications. Peritonitis caused by A xylosoxidans can disrupt PD treatment and pose challenges in its management. Removal of the PD catheter and transition to intermittent hemodialysis may be necessary to prevent the relapse of these infections. In our case reporting peritonitis caused by A xylosoxidans in patients undergoing PD, we observed a relapse of infections caused by A xylosoxidans, whereby the treatment regimen was changed to antibiotics that A xylosoxidans is susceptible to. Limited evidence on specific treatments, multidrug resistance, and the presence of other medical conditions further complicate the management of A xylosoxidans infections. Further research is needed to better understand the epidemiology, risk factors, clinical implications, optimal treatment strategies, and long-term outcomes associated with peritonitis caused by A xylosoxidans in patients undergoing PD.
Footnotes
Acknowledgements
The authors are grateful to the hospital staff for their contribution to the successful management and treatment of the patient.
Author Contributions
Ibrahim Tawhari: Conceptulaization; supervision.
Samantha Saggese: Writing—case presentation.
Shatha S. Alshahrani and Ghufran Asiri: Resources; writing—original draft.
Shatha A. Alshahrani and Sarah Summan: Resources; writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for the publication of case reports or case studies.
Informed Consent
The patient’s consent was obtained for the publication of their anonymized information in this article.