
Abstract
The purpose of this study was to summarize the pathogens that cause peritoneal dialysis (PD)-associated peritonitis and to identify risk factors for PD-associated peritonitis. This retrospective study included 115 end-stage renal disease (ESRD) patients receiving PD therapy. Patients were categorized into two groups: peritonitis group (n = 41) and non-peritonitis group (n = 74). Clinical data and laboratory tests were collected from medical records. The multivariate logistic regression model was used to evaluate associations between PD-associated peritonitis and potential risk factors. PD-associated peritonitis occurred 54 times in 41 patients. The most frequently identified pathogen was Gram-positive cocci (57.78%). Multivariate logistic regression analysis showed that serum albumin (β = –0.208, P < 0.001), blood phosphorus concentration (β = –1.732, P = 0.001), gastrointestinal disorders (β = 1.624, P = 0.043), and use of calcitriol (β = –2.239, P = 0.048) were significantly correlated with PD-associated peritonitis. Receiver operating characteristic (ROC) curves showed that the areas under the curve were 0.832 for serum albumin and 0.700 for blood phosphorus concentration with optimal cut-off values of 29.1 g/L for serum albumin and 1.795 mmol/L for blood phosphorus concentration. Gram-positive coccus is the major pathogen responsible for PD-associated peritonitis. Serum albumin <29.1 g/L, blood phosphorus concentration <1.795 mmol/L, and intestinal disorders are risk factors for PD-associated peritonitis, whereas the use of calcitriol can reduce the risk of PD-associated peritonitis.
Keywords
Introduction
Peritoneal dialysis (PD), hemodialysis (HD), and kidney transplantation are the renal replacement therapy options for patients with end-stage renal disease (ESRD). PD is the most common home dialysis option for ESRD patients. At present, more than 190,000 patients have received PD. 1 PD has been well accepted by ESRD patients because it has some advantages over HD, including good quality of life, increased preservation of residual renal function, high clearance of middle-sized molecules, low rate of hepatitis infection, and increased hemodynamic stability.
PD is associated with many complications including catheter tip migration, hypoproteinemia, peritonitis, plural effusions, and water and electrolyte disturbance. PD-associated peritonitis is a major complication that can lead to poor dialysis and reduced quality of life. Severe and repeated peritonitis can result in dysfunction of the peritoneal membrane, thus leading to PD failure and even death. Although the use of strict aseptic technique can reduce the risk of PD-associated peritonitis, it cannot prevent peritonitis. Several studies have reported that PD-associated peritonitis is associated with irreversible factors such as race, female, chronic pulmonary disease, coronary heart disease, hepatitis C, and diabetes2–5 as well as reversible factors such as nutritional deficiency, obesity, smoking, psychological factors, low socioeconomic status, and change from HD to PD.2,3,6,7 Therefore, it is important to identify and control risk factors for PD-associated peritonitis in order to reduce PD-associated mortality.
As to the pathogens of PD-associated peritonitis, the recommended target for culture-negative peritonitis episodes is ⩽15% set by the International Society for Peritoneal Dialysis (ISPD). 8 The most frequently identified Gram-positive coccus was Staphylococcus epidermidis. 9
In this study, we retrospectively reviewed the clinical data of 115 ESRD patients who received PD therapy in our hospital between 2009 and 2013 and summarized the pathogens responsible for PD-associated peritonitis in these patients. The purpose of this study was to identify risk factors for PD-associated peritonitis, and the results provide valuable clinical information for preventing PD-associated peritonitis and improving survival among PD patients.
Materials and methods
Patients
This study included 115 ESRD patients who received PD therapy in our hospital between 2009 and 2013. All patients received PD solutions (Baxter Co., USA). Dianeal were used for all patients. No patients were treated with Nutrineal and Extraneal. All the patients were on continuous ambulatory peritoneal dialysis (CAPD) and did not receive immunosuppressive therapy when they began to perform PD. Patients were categorized into two groups according to the presence of peritonitis after PD: peritonitis group (n = 41) and non-peritonitis group (n = 74). As to catheter implantation and patient’s training, special doctors and special nurses performed them in our hospital. So, in these two aspects, the two groups should not have differentiations. This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Jilin University. There was a statement to the effect that all subjects gave informed, signed consent to participate in the study, or in the case of children or deceased, informed written consent was given by the family or guardian.
Inclusion criteria
(a) Residence within the city and (b) receipt of PD therapy for more than 2 years. All patients did not share a PD room with others and received PD alone or in the presence of their relatives.
Exclusion criteria
(a) Residence in a rural and suburban area and (b) receipt of PD from PD operators who were not well trained (patients were not trained for >1 week by special nurses). PD-associated peritonitis was diagnosed based on two of the following three criteria according to the guidelines recommended by the International Society for Peritoneal Dialysis: 8 (a) abdominal pain and/or the presence of purulent drainage with or without fever; (b) white blood cell counts >100 per microliter with leukocytes accounting for >50% of polymorphonuclear leukocytes in PD effluents; and (c) positive bacteria culture results from PD effluents.
There is no consensus regarding the definition of intestinal bacteria, and thus, in this study, we included both enteric bacillus and enteric coccus.
Clinical data
Clinical data were collected from patients’ medical records, including age, gender, causes of ESRD, coronary heart disease, cerebrovascular diseases, gastrointestinal disorders (such as diarrhea and constipation), hepatitis C, history of smoking and drinking, dialysis status before PD, bacterial culture results from PD effluents, and the use of calcitriol. Laboratory tests including serum albumin, hemoglobin, serum creatinine, blood Ca2+ and phosphate, and parathyroid hormone (PTH) were reviewed.
Statistical analysis
Analyses were performed using SPSS17.0 (SSPS, Inc., Chicago, IL, USA). Numerical data are expressed as median and range (minimum and maximum) and compared with nonparametric tests. Categorical data were compared with Pearson chi-squared tests. The multivariate logistic regression model was used to identify associations between PD-induced peritonitis and potential risk factors. The cut-off values for determining PD-induced peritonitis were assessed using receiver operating characteristic (ROC) curves. Probability values ⩽0.05 were considered statistically significant.
Results
Clinical data
In the peritonitis group, PD-associated peritonitis occurred 54 times in 41 patients (17 men and 24 women). The causes of ESRD included chronic glomerulonephritis in 19 cases (20.4%), diabetic patients in 11 cases (20.4%), and other kidney diseases in 24 cases (44.4%), including 8 cases with chronic interstitial nephritis, 10 cases with hypertensive nephropathy, 2 cases with pyelonephritis, and 4 cases with unknown causes. Before the presence of PD-associated peritonitis, diarrhea occurred in 8 cases and constipation occurred in 3 cases. Diarrhea often occurred 1 day before peritonitis and constipation were often habitual. The non-peritonitis group included 74 patients (34 men and 40 women) who did not have PD-associated peritonitis for more than 2 years. The causes of ESRD included chronic glomerulonephritis in 22 cases (29.7%), diabetic patients in 23 cases (31.1%), and other kidney diseases in 29 cases (39.2%), including 10 cases with chronic interstitial nephritis, 11 cases with hypertensive nephropathy, 3 cases with pyelonephritis, 2 cases with polycystic kidney, 1 case with lupus nephritis, 1 case with purpura nephritis, and 1 case with unknown causes. Diarrhea occurred in 5 cases and constipation occurred in 2 cases.
Table 1 summarizes the clinicopathological features of patients in the peritonitis and non-peritonitis groups. There were significant differences in the use of calcitriol and the presence of diarrhea or constipation between the non-peritonitis and peritonitis groups (P < 0.05). There were no significant differences in patient age, sex, hepatitis C infection, etiology, smoking status, PD status, history of coronary heart disease, and history of cerebrovascular disease.
The clinicopathological features of patients in the non-peritonitis and peritonitis groups.

PD: peritoneal dialysis; HD: hemodialysis.
P < 0.01; *P < 0.05.
Pathogens
Table 2 summarizes the pathogen culture results for PD effluents from patients with PD-associated peritonitis. Of 54 pathogen cultures, positive results were found in 45 cultures (83.33%), including 26 (57.78%) cultures with Gram-positive cocci, 12 (26.67%) cultures with Gram-negative bacilli, and 7 (15.56%) cultures with fungi. Of the 12 cultures with Gram-negative bacilli, 11 cultures were enteric bacillus. Of the seven cases with fungal infection, primary fungal infection occurred in only one case, and infection secondary to bacteria occurred in the other six cases. The most frequently identified Gram-positive coccus was Staphylococcus epidermidis (7 cases), and the most frequently identified Gram-negative bacillus was Escherichia coli (6 cases).
The pathogen culture results for PD effluents in patients with PD-associated peritonitis.

PD: peritoneal dialysis.
Associations between PD-associated peritonitis and laboratory test results
Table 3 summarizes the laboratory results for patients with the non-peritonitis and peritonitis groups. There were significant differences in the serum concentrations of albumin, hemoglobin, blood phosphorus, and PTH between the non-peritonitis and peritonitis groups (P < 0.05). There were no significant differences in the serum creatinine and blood calcium concentrations between the two groups (P > 0.05).
The laboratory results for patients in the non-peritonitis and peritonitis groups.
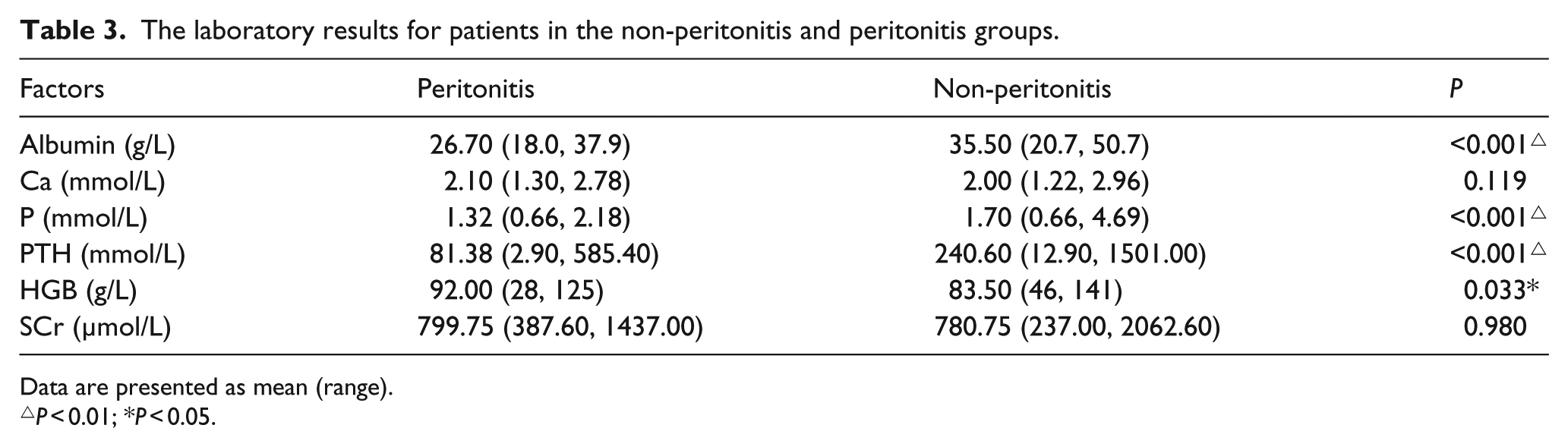
Data are presented as mean (range).
P < 0.01; *P < 0.05.
We further used the multivariate logistic regression model, including factors such as gastrointestinal disorders, use of calcitriol, serum albumin, hemoglobin, blood phosphorus concentration, and PTH, for predicting PD-associated peritonitis. Based on the multivariate logistic regression analysis, hemoglobin and PTH were not significantly associated with PD-associated peritonitis (P > 0.05). Serum albumin (β = –0.208, P < 0.001), blood phosphorus concentration (β = –1.732, P = 0.001), gastrointestinal disorders (β = 1.624, P = 0.043), and use of calcitriol (β = –2.239, P = 0.048) were significantly associated with PD-associated peritonitis (Table 4).
Multivariate logistic regression analysis of the risk factors for PD-associated peritonitis.

CI: confidence interval; OR: odds ratio; SE: standard error.
P < 0.01; *P < 0.05.
ROC curve analysis was used to assess the ability of the laboratory test results to predict PD-associated peritonitis (Figure 1). The area under the curve (AUC) was calculated for serum albumin and blood phosphorus concentrations, and the optimal cut-off value was determined (Table 5). The AUCs were 0.832 for serum albumin and 0.700 for blood phosphorus concentrations. The optimal cut-off values for predicting PD-associated peritonitis were 29.1 g/L (sensitivity = 85.1% and specificity = 72.2%) for serum albumin and 1.795 mmol/L (sensitivity = 93.9% and specificity = 43.8%) for blood phosphorus concentrations (Figure 1, Table 5).

ROC curves for the ability of serum albumin and blood phosphorus concentrations to predict PD-associated peritonitis.
The optimal cut-off values for serum albumin and blood phosphorus concentrations for predicting PD-associated peritonitis.

AUC: area under the curve; CI: confidence interval.
Discussion
Peritonitis is a common PD-associated complication that can lead to hospitalization and PD failure. The main cause of PD-associated peritonitis is due to inappropriate handling. However, many risk factors can increase the susceptibility of PD patients to peritonitis. In this study, we found that serum albumin and blood phosphorus concentrations in addition to diarrhea or constipation were risk factors for PD-associated peritonitis. The identification and control of risk factors for PD-associated peritonitis are important for the prevention and treatment of PD-associated peritonitis.
PD-associated peritonitis can be caused by many pathogens, such as bacteria and fungi. In this study, 9 (16.67%) of the 54 pathogen cultures were negative, and this negative pathogen culture rate is consistent with the recommended target for culture-negative peritonitis episodes is ⩽15% set by the International Society for Peritoneal Dialysis (ISPD). 8 In addition, we found that the most frequent pathogen was Gram-positive cocci (57.78%), followed by Gram-negative bacilli (26.67%). The most frequently identified Gram-positive coccus was Staphylococcus epidermidis, and the most frequently identified Gram-negative bacillus was Escherichia coli. These results are consistent with those of previous reports in the literature.9–11 PD-associated peritonitis caused by Gram-positive coccus is mainly due to inappropriate PD handling. In this study, all patients who were trained for appropriate use of PD lived in the city and did not share a room with others. However, Gram-positive coccus was still the most common pathogen responsible for PD-associated peritonitis in our patients. Therefore, it is important to thoroughly train every PD operator to improve appropriate PD handling. In addition, enterobacteria-associated peritonitis commonly occurs in patients with intestinal disorders or diabetes. Moreover, diabetes patients often have intestinal disturbance, chronic inflammation, or nutritional deficiency, which can lead to diarrhea or constipation. Therefore, PD-associated peritonitis caused by enterobacteria is commonly observed in patients with diarrhea or constipation.
For PD-associated peritonitis, fungal infection is relatively rare. Fungal peritonitis is severe and usually occurs only after the use of broad-spectrum antibiotics for the treatment of bacterial peritonitis. In this study, we found that fungal infection occurred in 7 (15.56%) of 54 cultures, which was higher than rates (3%–6%) reported in the literature. 12 The high incidence rate of fungal infection in this study is likely secondary to repeated bacterial infection, because 6 of 7 cases with fungal peritonitis were secondary to repeated bacterial infection. Primary fungal infection occurred in only one case. These findings suggest that PD patients with repeated bacterial peritonitis are susceptible to fungal infection. We thought that the relatively large number of patients with fungal peritonitis may be associated with secondary after antibiotic treatment.
Malnutrition is a common complication in PD patients and is closely associated with PD incidence and mortality. 13 The serum albumin concentration has been recommended by the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQ) for assessing the nutritional status of patients. 14 In this study, we found that the serum albumin concentration was significantly correlated with PD-associated peritonitis. ROC curves showed that the AUC was 0.831, and the optimal cut-off value for predicting PD-associated peritonitis was 29.1 g/L (sensitivity = 85.1% and specificity = 72.2%), suggesting that serum albumin can predict the risk for PD-associated peritonitis. Furthermore, multivariate logistic regression analysis showed that the serum albumin level was negatively associated with PD-associated peritonitis (β = −0.208, odds ratio (OR) = 0.812), suggesting that a low level of serum albumin is associated with a higher risk for PD-associated peritonitis. However, it remains controversial whether serum albumin is associated with peritonitis. Consistent with our findings, Ozturk et al. 15 reported that a decrease in serum albumin is associated with an increased risk for PD-associated peritonitis. In contrast, several other studies have shown that serum albumin is not correlated with PD-associated peritonitis.16,17 Based on our findings, correction of malnutrition, increased protein intake, and improved appetite are important for preventing and treating PD-associated peritonitis.
However, whether correction of malnutrition can reduce the incidence and mortality of PD-associated peritonitis remains unclear. Malnutrition is the result of a loss of protein and amino acids in the dialysis effluents. PD patients can lose 1–3.5 g/day amino acids and 5–10 g/day protein including albumin, immunoglobulin, transferrin, β2 microglobulin, and α2 macroglobulin, and this protein loss is increased during peritonitis.18–20 It has been reported that serum albumin is associated with the loss of albumin via the peritoneum and by inflammation, but the two processes were independent. 21 It has been reported that 1.1% amino acid PD solutions containing nine essential amino acids, six non-essential amino acids, and 40 mmol/L lactic acids can promote protein synthesis, maintain positive nitrogen balance, and increase body weight.22,23 However, the amino acid-containing PD solution can result in anorexia and metabolic acidosis as well as increased serum urea levels. Therefore, the best regimes for PD solutions and the amounts of supplemented amino acids remain to be determined in future studies.
Vitamin D deficiency is commonly found in patients with Stages 3–5 chronic kidney disease (CKD), especially those receiving PD. 24 Loss of vitamin D in PD effluents contributes to vitamin D deficiency in these patients. An epidemiological study has shown that CKD patients receiving vitamin D and its analogs exhibit increased survival. 25 In this study, multivariate logistic regression analysis showed that the use of calcitriol was negatively associated with PD-associated peritonitis (β = −2.239, OR = 0.107), suggesting that the use of calcitriol reduced the incidence of PD-associated peritonitis. This effect may be explained by the multiple biological activities of vitamin D, including the promotion of cell differentiation, inhibition of cell growth, and modulation of the immune system. However, the association between use of vitamin D and PD-associated peritonitis has not been well investigated, and the sample size of the study is relatively small. 26 Future studies with a large sample size are required to confirm our findings that the use of calcitriol reduces the risk of PD-associated peritonitis.
CKD patients commonly have hyperphosphatemia, which can lead to secondary hyperparathyroidism, excessive deposition of calcium and phosphorus, disrupted vitamin D metabolism, and renal osteodystrophy. In this study, we found that blood phosphorus concentrations were significantly correlated with PD-associated peritonitis. ROC curves showed that the AUC was 0.700, and the optimal cut-off value for predicting PD-associated peritonitis was 1.795 mmol/L (sensitivity = 93.9% and specificity = 43.8%), suggesting that blood phosphorus concentration can predict the risk for PD-associated peritonitis. Furthermore, logistic regression analysis showed that blood phosphorus concentrations were negatively correlated with PD-associated peritonitis (β = −1.732, OR = 0.177), suggesting that low blood phosphorus concentrations are associated with a higher risk for PD-associated peritonitis. The association between hypophosphatemia and PD-associated peritonitis has not been reported, and further studies with a large sample size are required to confirm our findings. One explanation for the inverse relationship between serum phosphorous and peritonitis incidence may be the association between malnutrition and low blood phosphorous concentration.
In this study, we found that diarrhea or constipation occurred in 11 (20.37%) of 54 cases in the peritonitis group, and in 7 (9.46%) of 74 cases in the non-peritonitis group. Thus, diarrhea or constipation occurred more frequently in the peritonitis group than in the non-peritonitis group, suggesting that gastrointestinal disorder is a risk factor for PD-associated peritonitis. Furthermore, multivariate logistic regression analysis showed that diarrhea and constipation were positively correlated with PD-associated peritonitis (β = 1.694, OR = 5.439), suggesting that the presence of diarrhea or constipation increases the risk for PD-associated peritonitis. It has been reported that peritonitis can be caused by transmural migration of intestinal microbes. 27 In ESRD patients with uremia, the intestinal wall exhibits pathological changes that allow microbes to enter the abdominal cavity to induce peritonitis via the lymph nodes or intestinal wall during intestinal infection and diarrhea or constipation. Constipation is very common in ESRD patients, but is often ignored. It is important to guide PD patients to defecate normally in order to prevent constipation and thereby reduce the incidence of peritonitis caused by intestinal microbes.
In summary, we analyzed risk factors for PD-associated peritonitis and found that serum albumin <29.1 g/L, blood phosphorus concentration <1.795 mmol/L, and intestinal disorders were risk factors for PD-associated peritonitis. The use of calcitriol reduced the risk of PD-associated peritonitis. Our study suggests that improvement of serum albumin and blood phosphorus concentrations, prevention or treatment of diarrhea and constipation, and use of calcitriol can reduce the occurrence of peritonitis in PD patients. Further studies with a large sample size across multiple centers are required to confirm our findings.
Footnotes
Acknowledgements
H.W. and X.W. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.