
Abstract
There have been studies published regarding the association between developing Brugada syndrome after an acute COVID-19 infection. In this case, we present a patient who presented with a syncopal episode and subsequently found to have Type I Brugada pattern on electrocardiogram. The patient underwent placement of a single chamber defibrillator. Genetic analysis demonstrated SCN5A variant which is associated with cardiac conditions including Brugada syndrome.
Introduction
Acute COVID-19 infection has been found to cause myocarditis and associated life-threatening arrhythmias. 1 It has been cited that this infection could unmask underlying channelopathies in the presence of elevated inflammatory markers without the presence of fever. Multiple case reports have been published regarding patients developing Brugada syndrome after an acute COVID-19 infection.2,3 However, there are no case reports to discuss a possible relationship between Brugada syndrome and the COVID-19 vaccine. In this case, we explore a patient who presented with syncope, likely Brugada-induced, and possibly related to the Moderna COVID-19 vaccine.
Case Summary
A 56-year-old male with no known cardiac history presented to the emergency room for recurrent syncopal episodes. He received the Moderna COVID-19 vaccine booster at noon the day prior to the emergency room visit. Earlier in the day that he received the vaccine, he took his daily paroxetine at 8:00
In the emergency room, the patient had a heart rate of 75 beats/minute and blood pressure of 156/97 mmHg, temperature 37.4C, respiratory rate 15 breaths/minute. Cardiac examination revealed normal radial and carotid pulses, normal S1 and S2, without added sounds or murmurs. His lab work including complete blood count, metabolic panel, cardiac biomarkers, and D-dimer were negative. His electrocardiogram (ECG) demonstrated elevation of the J point, a coved-type ST segment, and an inverted T wave in V1 and V2 concerning for Type I Burgada Pattern (Figure 1), all of which were new findings compared with a prior ECG in 2018 which did not show Brugada pattern (Figure 2).
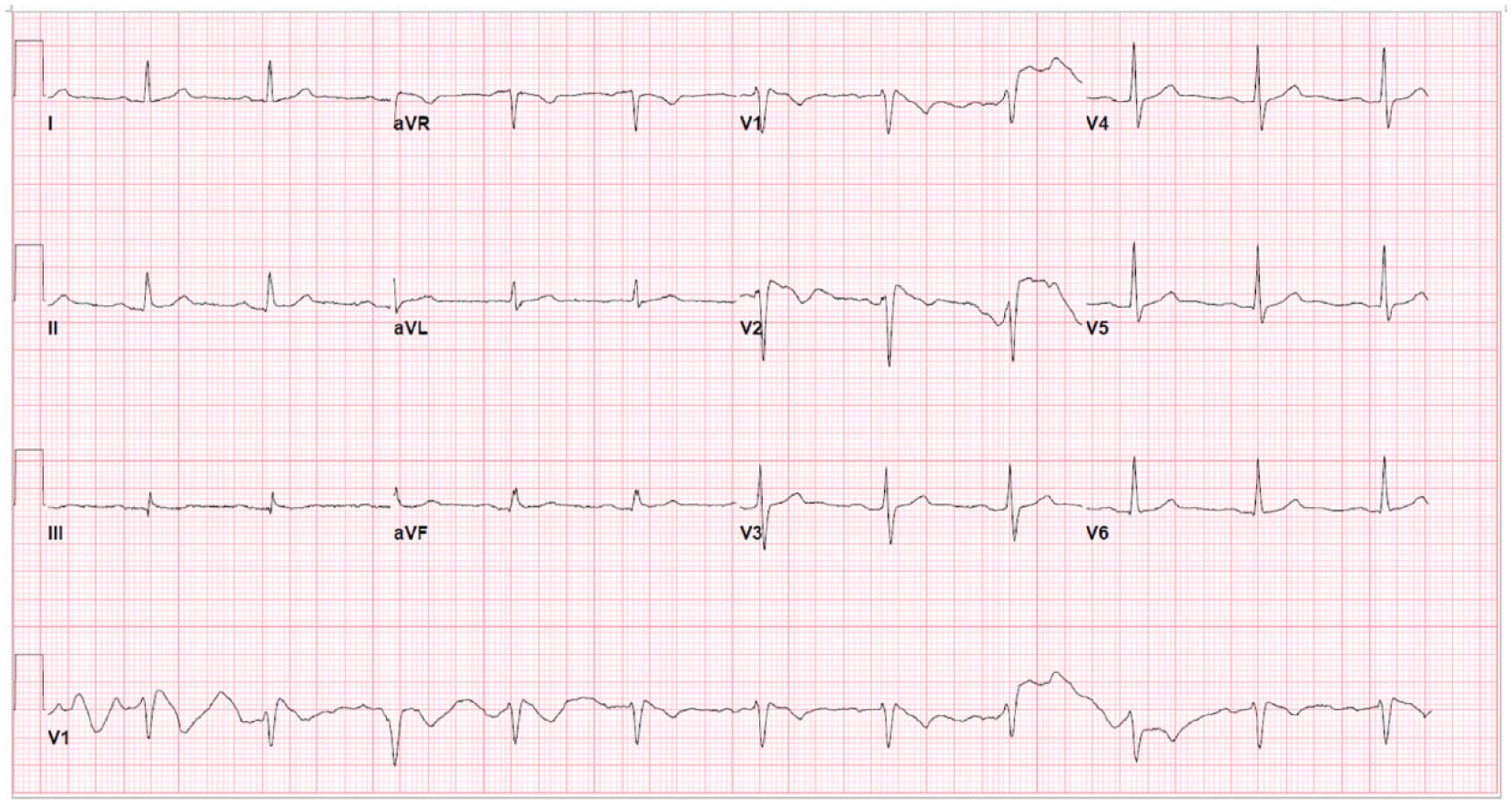
Sinus rhythm with first-degree atrioventricular block and Brugada Type I.
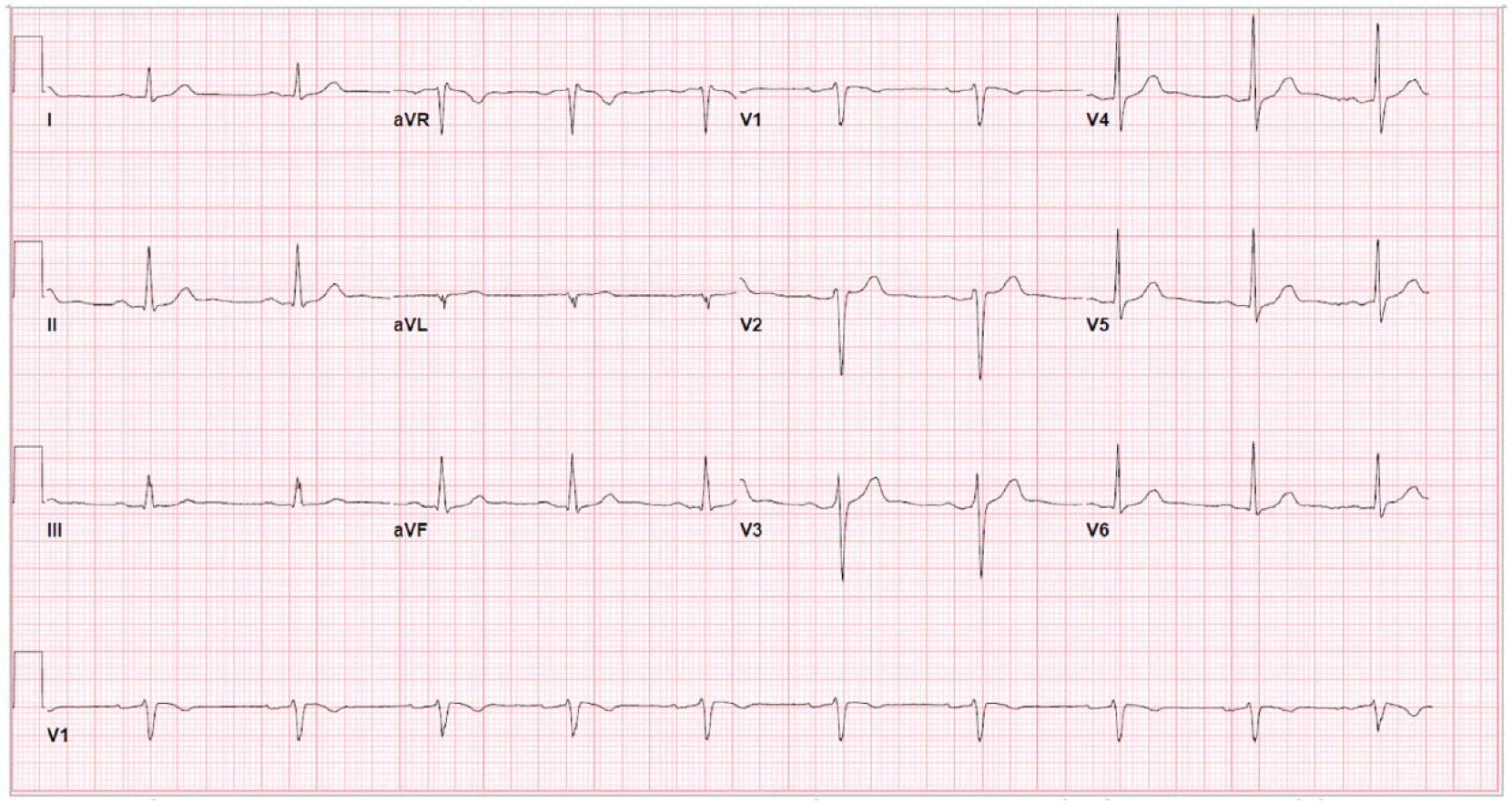
Sinus rhythm with first-degree atrioventricular block and loss of Brugada pattern (before Moderna COVID-19 vaccine).
Given these findings, the cardiology service was consulted. A transthoracic echocardiogram showed normal left ventricular size, normal left ventricular wall thickness and normal left ventricular systolic function. There was mild tricuspid insufficiency, trace to mild mitral insufficiency, and mild aortic insufficiency. In view of the otherwise unexplained syncopal event and Brugada pattern on ECG, the patient was taken to the electrophysiology lab to have a single chamber defibrillator implanted, performed without complications. Repeat ECG after implantation of the single chamber defibrillator demonstrated the patient remained in sinus rhythm with first-degree AV block without Brugada pattern (Figure 3). Subsequent genetic testing showed variant of SCN5A which is associated with autosomal dominant cardiac conditions including Brugada syndrome, long QTc syndrome, dilated cardiomyopathy, and atrial fibrillation. 4
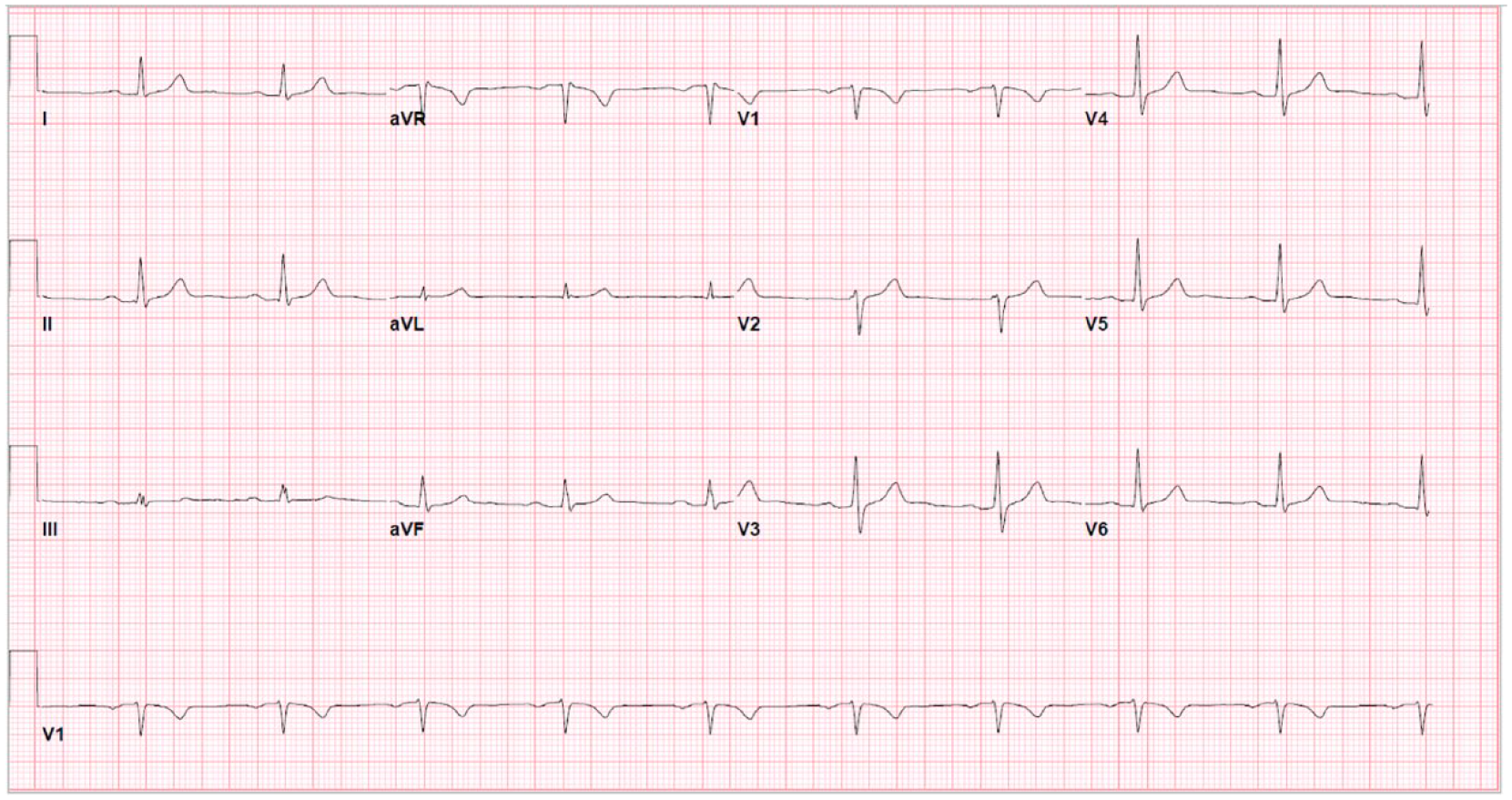
Sinus rhythm with first-degree atrioventricular block status post-implantable cardioverter-defibrillator with resolution of Brugada Type I.
Discussion
Type I Brugada is characterized by elevation of the J point, a coved-type ST segment, and an inverted T wave in V1 and V2. 5 These changes are not linked to any evidence of ischemia, electrolyte abnormalities, or other structural heart disease. Brugada syndrome is defined as an inherited channelopathy associated with increased risk for sudden cardiac death secondary to arrhythmias. Patients who are asymptomatic with Brugada pattern on ECG carry a higher risk of VF than healthy individuals. 5
After a thorough review of the patient’s medical history and prior ECG, we concluded that the patient’s presentation of recurrent syncopal episodes and new ECG findings compatible with Brugada syndrome were unmasked by the Moderna COVID-19 Vaccine Booster. To our knowledge and literature review, this has not occurred before. Our patient underwent genetic testing, which confirmed a positive SCN5A mutation for Brugada syndrome. Sodium channel genes (SCN) encode subunits of a cardiac sodium channel. There are 2 known sodium channel gene mutations responsible for the possibility of Brugada syndrome, including SCN5A and SCN10A. These myocardium sodium channels, if defective, will reduce sodium inflow currents, thus reducing the duration of a normal action potential.4,6 When analyzing an ECG of a patient with Brugada syndrome, as mentioned above, there is ST segment elevation and T wave inversions of the right precordial leads. The pathophysiology behind this phenomenon is not clearly understood; however, it is thought to affect the ventricular myocardium, specifically the action potentials of both epicardial and M cells. Despite endothelial cells being a component of the ventricular myocardium, these cells have not been deemed responsible for the ECG changes of Brugada syndrome.4-6
Regarding this patient, genetic testing was positive for a mutation in SCN5A. The gene encodes specifically the Nav1.5 subunit of the cardiac sodium channel gene on chromosome 3p21-24 which is found to affect about 20% to 30% of those with Brugada syndrome. This gene is associated with autosomal dominant Brugada syndrome in addition to long QT syndrome, dilated cardiomyopathy, and atrial fibrillation. The mutation is described as a “loss of function” mutation and can result in several manifestations including lack of expression, variance regarding voltage and time dependent of activation, and either prolonged or accelerated recovery from inactivation.4,5 Given current guidelines, since the patient presented with a history of recurrent syncope which was otherwise unexplained and was associated with the Brugada pattern, the patient was treated with an implantation of an implantable cardioverter-defibrillator.
The phenotypic expression of Brugada syndrome can be unmasked during febrile illnesses. We have presented a novel case in which COVID-19 vaccine may have precipitated an arrhythmic event in a patient with previously unknown genotype positive Brugada syndrome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.