
Abstract
Neuroretinitis, originally described by Leber at the turn of the 20th century, has long perplexed ophthalmologists due to its multiple recognized causes and often atypical presentation. Optic disk edema and macular star in the affected eye are well-agreed upon findings and are due to increased permeability of blood vessels near the optic disk and in the retina at large. It also is universally painless and presents with a relative afferent pupillary defect (RAPD) in the affected eye or eyes. However, depending on the infectious agent, an underlying autoimmune condition, or undefined idiopathic cause, there can be various degrees of vision loss, visual field loss, progression or recurrence, as well as involvement of the other eye. We present this case of presumed sequential idiopathic neuroretinitis with severe vision and visual field loss with a low-positive anti-MOG test in the border county of El Paso.
Background
Idiopathic neuroretinitis (INR) is an inflammatory condition, presumed autoimmune, that is sometimes considered a form of papillitis. It arises as inflammation around the blood supply of the optic disk leads to increased permeability and edema of the optic disk, as well as subsequent edema of different regions of the retina. Owing to the inflammatory nature of the condition, it is more likely to present with cells in the vitreous compared to other conditions affecting the anterior optic nerve (ON), such as non-arteritic anterior ischemic optic neuropathy (NAION). 1 It usually presents with painless unilateral visual acuity (VA) loss, visual field (VF) loss, commonly central scotoma, as well as a relative afferent pupillary defect (rAPD) in the affected eye. Some early signs include optic disk edema, chorioretinal white spots, hemorrhage, or cotton wool spots in the peripapillary area. Without treatment, the retina outside of the peripapillary area becomes involved (macular/retinal edema, exudates, and retinal detachments). 2
Although the most common cause of neuroretinitis (NR) is infectious (Bartonella henselae), recurrent or sequential NR tends to be idiopathic. 3
Case Report
A 44-year-old White man with hypertension presented to ophthalmology with complaints of acute painless VF loss in the inferior hemifield that progressed to complete VA/VF loss in the right eye (OD), accompanied by headaches and occasional flashes of light. At the time of initial presentation at a comprehensive ophthalmology office in late September 2021, the patient was hypertensive at 150/100 mm Hg with best-corrected VA (BCVA) in the right eye (OD) 20/200, and BCVA left eye (OS) 20/20, no rAPD reported. Fundus exam showed optic nerve edema OD and a small cup-to-disk ratio (CDR) OS of 0.1. The patient was referred to neurology who reported unremarkable brain MRI and a lumbar puncture (LP) with low opening pressure <13 cm H2O. The patient was started on high-dose oral prednisone by the neurologist after lumbar pucture; 1250 mg for 3 days and tapered over 11 days with only objective improvement of VF.
Same week, patient was then seen by neuro-ophthalmology. His headaches had resolved, but he complained of intractable hiccups and overall fatigue; his BCVA OD was now 20/350, with color desaturation and rAPD OD. Dilated fundus exam (DFE) showed right eye complete blurring of disk margins with blurring of exiting and central vessels, and supero-temporal paramacular edema, without complete “macula star.” Left fundus showed ON margins blurring at superior half margin with minimal blurring of exiting vessels with no blurring of central vessels with CDR of 0.05, and no macular edema. No hemorrhages, cotton wool spots (CWS), or inflammation was seen. The rest of the retina was unremarkable.
Optical coherence tomography (OCT) confirmed diffuse nerve head edema OD and trace ON edema and small CDR and tilt OS (Figure 1).
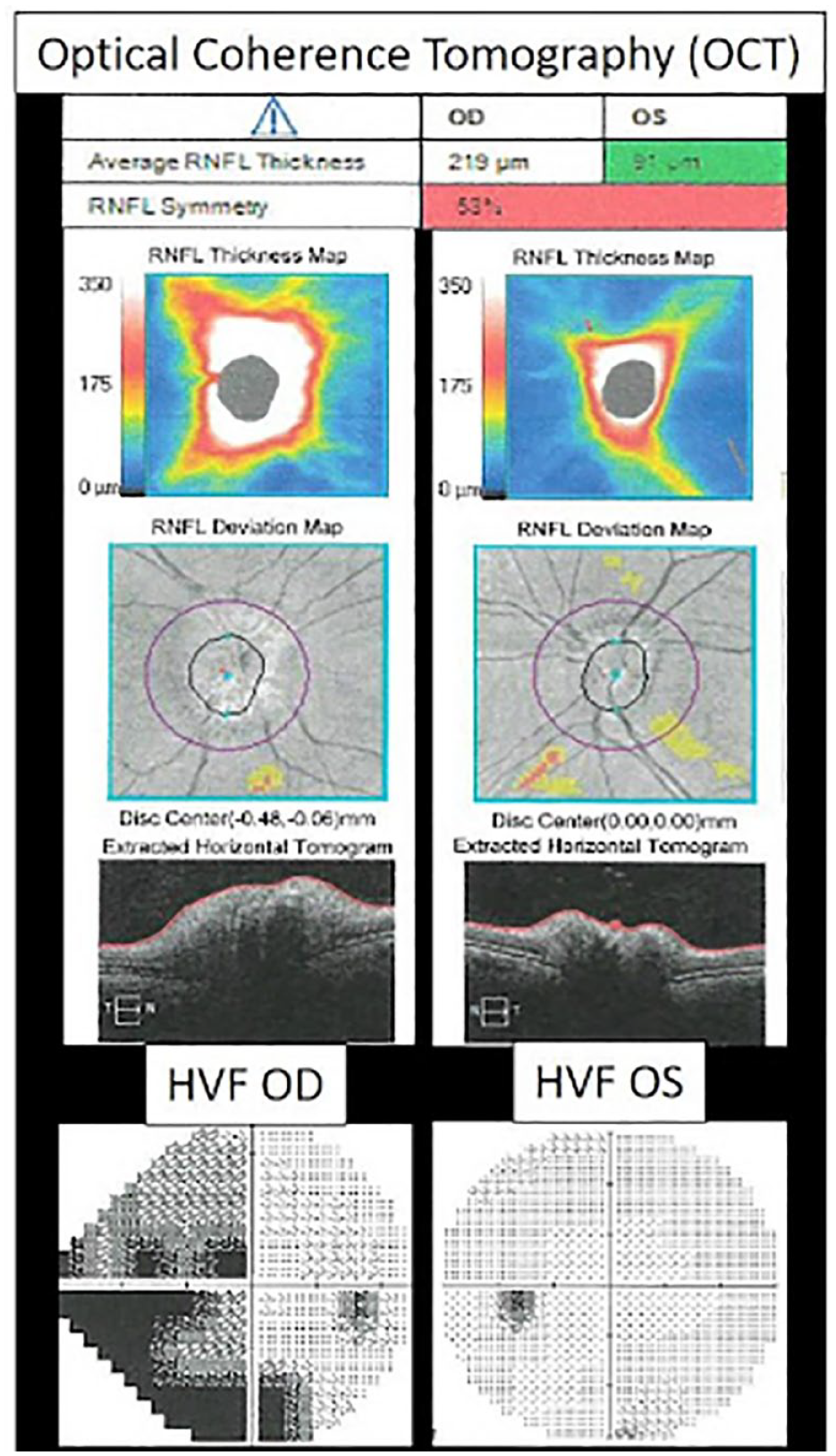
Initial exam. Optical coherence tomography (OCT) with quantification of optic nerve/retinal nerve fiber layer (RNFL) thickness edema right eye. No macular edema. Humphrey visual field (HVF) stimulus V 24-2 OD showing incomplete superior and inferior altitudinal defect OD; stimulus III 30-2 OS normal.
Visual field showed incomplete superior and inferior altitudinal defect OD. B-Scan showed no ON drusen or signs of posterior scleritis. His physical exam, including neurological and cranial nerve exam, was normal.
Based on this exam, it was determined that patient had optic nerve edema in both eyes, but more severe in the right than the left. The decision was made to admit him to the hospital for repeated MRI brain and orbit, brain MRV, and repeated lumbar puncture. Magnetic resonance imaging showed diffuse leptomeningeal enhancement and thickening without nodularity (Figure 2); MRV was unremarkable, and venous sinus thrombosis was ruled out. Lumbar puncture opening pressure was 10 cm H2O. Cerebrospinal fluid (CSF) analysis was traumatic and showed high protein of 166 (normal ≤60) and glucose 120 (serum glucose 99). Cerebrospinal fluid cultures were all negative. Extensive labwork was pertinent for neutrophilic leukocytosis (presumed from steroids), low serum ACE. Otherwise, unremarkable CBC, ESR/CRP, RPR, CSF VDRL, HIV, cryptococcal antigen, p-ANCA, c-ANCA, and Lyme Abs, negative AQ4 antibody and antiphospholipid panel. A full-body FDG PET showed no remarkable foci of increased avidity.

MRI orbits and brain. Upper panel shows MRI T2 high definition showing the right optic nerve head thickening (arrows). No enhancement or hyperintensity of nerve. Lower panel shows MRI brain T1 with contrast with positive nonspecific diffuse pachymeningeal thickening(arrow heads) without nodularity.
Because of intractable hiccups and leptomeningeal enhancement, the patient underwent MRI cervical and thoracic spine with and without contrast, and no demyelinating lesions were found.
He received 1 gm methylprednisolone daily for 4 days and discharged with a 100 mg prednisone per day, and sent to neurology for immunosuppression.
Steroid treatment resolved headaches, intractable hiccups, and fatigue, and peripheral vision continued to improve OD. At this time, Anti-Myelin Oligodendrocytes antibody (MOG-Ab) from initial neurology work up resulted on a low-positive titer in serum (ELISA 1:20; Quest Diagnostic, San Juan Capistrano CA). While starting immunosuppression in early November 2021 (mycophenolate mofetil 250 mg BID PO), the patient stopped steroids and next day he woke up with acute inferior hemifield defect the left, contralateral eye.
Best-corrected VA was now 20/150 both eyes (OU). Fluorescein angiography (FA) while on immunosuppression showed normal flow throughout the retina and choroid. Repeated titers from a cell-based assay showed negative MOG-Ab (CBA; Quest Diagnostic, San Juan Capistrano CA). He was hospitalized for high-dose IV steroids and plasma exchange. Approximately one and a half months later, in December 2021, MOG titers were repeated following plasma exchange and stabilization of his condition. They were negative. The patient was still taking oral steroids, 100 mg daily for 2 months and was told not to taper down to 80 mg until February of 2022. Mycophenolate was also continued at this time.
Following these interventions and a 5-day hospitalization, best-corrected vision at follow-up appointments in mid to late 2022 was 20/60 OD, 20/70 OS. Final VF improved to having only a nasal inferior defect in both eyes. He has been relapse-free with mycophenolate mofetil 2g/day and prednisone 10 mg daily. Symptoms, imaging, and fundus findings since then have remained stable.
Discussion
Neuroretinitis usually presents with optic disk edema and development of macular star (even if incomplete). Causes for NR are seen in Table 1. The most common infectious cause is cat-scratch disease, while recurrent NR is most often idiopathic. 1
Causes of Neuroretinitis.

The worst visual outcomes tend to be associated with large RAPDs as well as slower resolution of optic disk edema. 4
We discuss this challenging case of sequential vision loss with initial leptomeningeal enhancement sensitive to steroids, presumed sequential INR.
Autoimmune demyelinating disease was initially suspected because of the patient’s young age and sex, “simultaneous and sequential” optic neuropathy presenting with edema, area postrema type symptoms—intractable hiccups, common in neuromyelitis optica (NMO) 6 headaches, leptomeningeal enhancement, and inflammatory CSF. The patient was treated with steroids and plasma exchange (PLEX). Neuromyelitis optic spectrum disorder (NMOSD) was tested for both NMO-aquaporin 4 Antibody and Myelin oligodendrocyte antibody disorder (MOGAD), resulting in weakly positive MOG-Ab serology.
MOGAD has been known to affect other than the optic nerve such a as macular edema, subhyaloid hemorrhage, 7 among others.8,9 This patient had supero-temporal paramacular edema, without complete “macula star” suspected to be only spread from optic nerve edema. The first low titer MOG-Ab ELISA was taken prior to steroid and mycophenolate. The second and third MOG-Ab were performed at MAYO clinic while the patient was already on mycophenolate, known to induce seronegativity faster than the regular course, as found by a study by a prospective study induced seronegativity 196.8 days vs 230.8 days without mycophenolate). 10 Although low-titer MOGAD was a considered possibility.
His entire clinical picture, including his lack of pain and optic nerve enhancement, minimal visual recovery after high dose IV steroids and plasma exchange, acute contralateral vision loss next day after stopping steroids, was not the typical progression of MOGAD. Furthermore, two neurologists and two neuroophthalmologists, one of them a MOGAD specialist concluded low-positive titers of anti-MOG Ab to be false positive (as it is in up to 50% of cases). 11 The follow-up serum MOG-Ab tests were taken while on steroids and mycophenolate and they were both negative. We remain open to the possibility of an atypical presentation of MOGAD but patient has had no relapses or new demyelinating disease presentation.
Even when imaging was not typical for NMOSD (long optic nerve demyelination, brain lesions), leptomeningeal enhancement and inflammatory CSF has been reported to rarely occur in NMOSD.12,13 He was treated with multiple PLEX treatments,12,14 but he showed minimal resolution.
Multiple repeated labwork was unremarkable, and PET showed no active lymph nodes, making sarcoidosis a less likely diagnosis.
An uncommon cause of bilateral asymmetric NR is Vogt-Koyanagi-Harada disease (VKHD) which would also present with meningitis in the early phases; however, our patient showed no retinal vascular abnormalities or retinal pathology on FA except from sectorial macular edema OD at onset.
The final consensus diagnosis was recurrent INR, most likely autoimmune MRI abnormalities in NR have been shown before; however, they are not the norm. These findings most commonly include intraocular optic disk enhancement at the nerve-globe junction as well as optic nerve and optic nerve sheath enhancement. This patient, like most patients with NR, did not have these findings on MRI. 15 Magnetic resonance imaging may show minimal retrobulbar enhancement up to 4 mm beyond the globe. 4
Acute FA in NR commonly shows diffuse disk edema, peripapillary dye staining in the midvenous and late phases. 1
Idiopathic recurrent NR is best treated with long-term immunosuppression with agents like mycophenolate or azathioprine in addition to maintenance steroids. 3
Visual outcomes in INR vary from 20/20 to light perception. The worst visual outcomes tend to be associated with large RAPDs as well as slower resolution of optic disk edema- rather than the degree of involvement of the macula. 4 Recurrent and bilateral involvement show worse prognosis as well.
The most common cause of NR involves infectious agents, of which the most common is Bartonella henselae, the agent of cat scratch disease (CSD). Others include Toxoplasma gondii, Treponema pallidum, Borrelia burgdorferi, Leptospira interrogans, Rickettsia rickettsii, Mycobacterium tuberculosis, Salmonella enterica, and Toxocara canis.
Less-common causes are viruses, fungi, or pre-existing autoimmune disease (sarcoidosis, PAN, or IBD). Associated syndromes include IRVAN, TINU, Perry-Romberg, and DUSN syndrome (which is caused by Rickettsia rickettsii, Mycobacterium tuberculosis, Salmonella enterica, and Toxocara canis specifically). Infectious causes tend to only cause a single episode rather than recurrent disease and tend to present with mostly macular involvement and less optic nerve involvement (i.e. no RAPD), making the prognosis much better. 1 Cat scratch disease is the most common cause and is usually treated with rifampin, ciprofloxacin, doxycycline, or Bactrim.
According to studies, CSD NR after treatment showed visual outcomes of 20/40 or better in 93% of subjects, for an average lines gained of 7.7. 5 In general, recurrent NR tends to be idiopathic, with a presumed autoimmune cause and cumulative loss of nerve fiber layer with a much more guarded visual prognosis. It should be suspected if patient shows recurrent attacks with poor recovery and an RAPD, no constitutional symptoms, no specific infectious risk factors or travel. If the reverse is true, the patient likely has CSD NR and should have titers repeated in 6 weeks if initially negative. 1
Conclusion
This case was challenging due to its atypical presentation with many masqueraders in the differential diagnosis. Being vigilant with regard to exam, imaging, serology, and response to treatment can help identify idiopathic recurrent NR and initiate azathioprine or mycophenolate earlier in addition to steroids, preventing the optic disk edema that will progress to atrophy and cause permanent vision loss.
Footnotes
Acknowledgements
The authors thank Dr. Prospero Ponce for her unwavering patience and support in getting this case report published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
TTUHSC-EP does not require IRB approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.