
Abstract
Esophageal heterotopic gastric mucosal patches (HGMP), also known as cervical inlet patches (CIP), is a rare but underdiagnosed condition characterized by the presence of salmon-colored, velvety mucosa located in the proximal esophagus, distal to the upper esophageal sphincter. The incidence of CIP ranges from 3% to 10% in adults, and its endoscopic appearance is characterized by a flat or slightly raised salmon-colored patch. In this case, we report a 78-year-old man who presented with symptoms of laryngopharyngeal reflux and dysphagia. An esophagogastroduodenoscopy showed a flat area of salmon-colored patch between 17 and 20 cm from the incisors, suggestive of a CIP complicated by stricture. The biopsy results showed an oxyntic-type mucosa lined with columnar cells consistent with an inlet patch. Esophageal dilation was done with a savory dilator with no resistance at 18 mm. The patient was placed on maintenance acid suppression therapy with proton-pump inhibitors and reported complete resolution of symptoms at the 1-month follow-up.
Keywords
Introduction
Esophageal heterotopic gastric mucosal patches (HGMP), also known as cervical inlet patches (CIP), are a rare but underdiagnosed condition characterized by the presence of salmon-colored, velvety mucosa located in the proximal esophagus, distal to the upper esophageal sphincter in the postcricoid area. Cervical inlet patch is considered a congenital anomaly with ectopic gastric mucosa which can secrete acid into the esophagus and cause a variety of symptoms and complications. 1 The incidence of CIP ranges from 3% to 10% in adults, which is usually solitary and well-defined by its margins.1-3
In this case report, we present a patient with esophageal CIP who presented with symptoms of laryngopharyngeal reflux (LPR) and dysphagia. We discuss the pathogenesis, clinical features, associations, complications, diagnosis, treatment, and endoscopic findings of CIP. Our aim is to increase awareness of this underdiagnosed condition among health care professionals and to highlight the importance of recognizing and managing CIP in patients with throat symptoms.
Case Report
A 78-year-old man presented with a 2-year history of persistent dysphagia to solid food. He reported difficulty swallowing pills, a globus sensation, thick phlegm that was difficult to expectorate, and frequent coughing due to food getting stuck in his “throat.” The food and pills would eventually pass on their own within a few minutes, and he had no history of food impaction requiring endoscopic intervention. He did not experience difficulty swallowing liquids, odynophagia, or weight loss. Despite trying over-the-counter antacids and famotidine, his symptoms did not improve. He had no history of smoking or alcohol use and no family history of cancers. After an evaluation by an otolaryngologist, which showed unremarkable findings on direct laryngoscopy, he was referred to gastroenterology for further evaluation of his cough and dysphagia.
The patient had a similar episode of symptoms 7 years prior, and a barium swallow at that time showed mild contrast retention in the hypopharynx. The symptoms improved on their own within a few months with instructions to change meal habits, without the need for endoscopic intervention.
For his current symptoms, he underwent an esophagogastroduodenoscopy (EGD), which showed a flat salmon-colored patch, suggestive of a CIP, between 17 and 20 cm from the incisors, and pearly white mucosa in the remaining part of the esophagus (Figures 1 and 2). A circumferential stricture was found at 20 cm from the incisors.

Upper endoscopy demonstrating circumferential stricture.
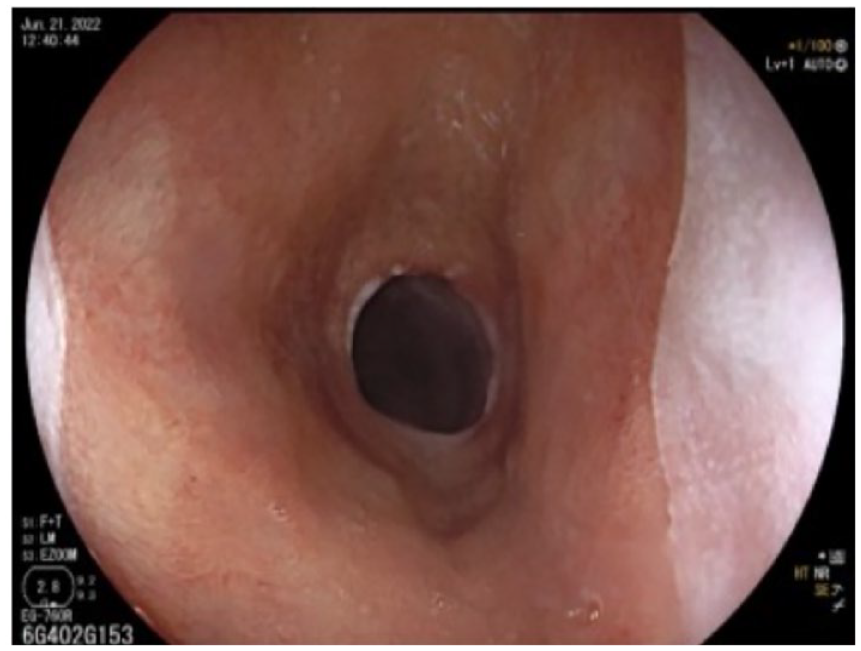
Upper endoscopy demonstrating circumferential stricture and cervical inlet patch along the upper esophagus.
The patient underwent esophageal dilation using a savory dilator without resistance at 18 cm, and multiple biopsies were collected. The biopsy results showed an oxyntic-type mucosa lined with columnar cells consistent with a CIP and were negative for intestinal metaplasia, eosinophilic esophagitis, viral inclusions, dysplasia, or malignancy. The rapid urease test and histology results were also negative for Helicobacter pylori.
After starting maintenance acid suppression therapy with proton-pump inhibitors (PPIs), the patient reported complete resolution of symptoms at the 1-month follow-up.
Discussion
Esophageal HGMP or CIP is a rare condition, located distal to the upper esophageal sphincter in the postcricoid area. The incidence of CIP ranges from 3% to 10% in adults1-3 and is often thought to be underdiagnosed with 1 study reporting that awareness of this condition could increase its endoscopic prevalence by 10-fold. 4
The origin of CIP is believed to be congenital, representing a remnant of the esophageal columnar mucosa that failed to be replaced by squamous lining during embryonic development. 1 This theory is supported by the presence of embryonic-type gastric mucosal characteristics found on immunohistochemical examination. 5 Another hypothesis suggests that the development of CIP may be a multistep process that results from the occlusion of esophageal glands and the formation of retention cysts, resulting in focal areas of HGMP. 6
Symptoms of CIP are often related to acid production and are nonspecific, including throat discomfort, globus sensation (nonpainful sensation of a lump in the throat), sore throat, hoarseness, odynophagia, and dysphagia.7,8 Cervical inlet patch is increasingly recognized as a cause of nonspecific throat symptoms believed to be due to LPR. 9 There have been reported cases of complications associated with CIP, such as bleeding, 10 perforation, 11 web, 12 stricture, 13 and adenocarcinoma. 14
Acid exposure below the inlet patch can lead to the development of esophageal stricture due to normal esophageal flow and gravity. Although some studies have reported a link between CIP and Barrett’s esophagus,15,16 many studies have not found evidence of this association. 9 CIP can be accompanied by other conditions, such as duodenal ulcers, reflux esophagitis, gastric polyps, and epiglottic cysts. 7
Studies have revealed that as much as 70% of patients with a colonized stomach can have H pylori colonizing their CIP, 17 and are significantly associated with globus sensation.7,16 However, our patient tested negative for H pylori.
Cervical inlet patch is diagnosed through endoscopic examinations, which detect well-differentiated, salmon-colored patches. However, due to proximal esophageal location, they can often be overlooked by endoscopists. The best examination of the proximal part of the esophagus is achieved when the endoscope is being withdrawn. A recent study showed that the endoscopic diagnosis yield for CIP can be increased 3-fold by using narrow-band imaging during the withdrawal of the endoscopy, compared with the traditional white light method.8,18
The main treatment for CIP is maintenance of acid suppression with PPIs or Histamine H2-receptor antagonists (H2RA). The mechanism of action is not known, but it may be due to acid suppression reducing inflammation and promoting the development of a squamous esophageal lining. Endoscopic therapy such as ablation of CIP using argon plasma coagulation (APC) has been shown to alleviate CIP-related symptoms, particularly globus sensation. 19
Our case is unique and noteworthy for several reasons. First, it highlights the presence of esophageal stricture as a complication of a potentially underdiagnosed condition, which is often missed by endoscopists. This is particularly significant as early detection and management can prevent the development of severe dysphagia and other complications. Second, the case demonstrates that CIP can present at any age, regardless of the presence of known risk factors such as Barrett’s esophagus, H. pylori infection, or dysplasia. Furthermore, our patient’s response to dilation and acid suppression therapy was consistent with previous studies, reinforcing the importance of early intervention in managing this condition. Finally, this case highlights the need for clinicians to consider CIP in patients presenting with laryngeal symptoms, globus sensation, and cough, and to manage the condition before it progresses to more serious complications such as esophageal stricture. Overall, this case is of interest to the medical community and underscores the need for heightened awareness of CIP and its potential complications.
Conclusion
Esophageal HGMP or CIP is a rare but underdiagnosed condition that can cause a variety of symptoms and complications. This case report highlights the importance of recognizing and managing CIP in patients with laryngopharyngeal symptoms and dysphagia. A prompt diagnosis and appropriate treatment with acid suppression therapy can result in resolution of symptoms. Health care professionals should be aware of this condition and consider it as a differential diagnosis in patients presenting with laryngopharyngeal symptoms and dysphagia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.