
Abstract
A 41-year-old woman showed a palpable mass at the superonasal orbital edge on the right side. Magnetic resonance imaging demonstrated a lobulated fluid-containing tubular mass which extended anteriorly to posteriorly along the medial orbital wall, nasal to the eyeball. She was followed once a year for 8 years until the age of 49 years when she decided to undergo surgical resection because of the enlarged mass. The lobulated large mass was resected and the pathology showed sparsely distributed spindle cells, positive for CD34, in alcian blue-positive mucous substances, indicative of myxoma. Postoperative magnetic resonance imaging showed residual lobulated tubular mass along the optic nerve on the medial side and superior to the eyeball. The residual orbital mass showed stable structure with more evident connection with the ethmoid sinus lesion, suggestive of the ethmoid origin, in 12 years until the age of 61 years. In the review of 20 patients with orbital myxomas in the literature, in addition to this case, roughly classified locations in the orbit were retrobulbar in 8 patients, on the lateral side of the orbit in 4, on the superior side in 6, on the medial side in 1 (this patient), and in the orbit with no specific description in 2. In pathological examinations, immunohistochemistry was not done in 8 patients, done but all negative in 2, and positive in 11 patients: nerve sheath myxoma was diagnosed in 3 patients based on positive S100 staining. Orbital myxoma is rare but considered in differential diagnosis of orbital masses.
Background
Myxoma is a rare benign neoplasm of primitive mesenchymal cells which are dispersed in mucous substances. Famous sites of the neoplastic origin are the atrium of the heart as cardiac myxoma1,2 and also the jaw bone as gnathic myxoma. In the field of the face and head, myxoma has been rarely detected in the orbit,3-22 cornea, 23 and conjunctiva24-27 of the ocular surface, eyelid,28-30 nasal cavity, and paranasal sinuses.31-40 We experienced a patient with orbital myxoma who showed connection with the ethmoid sinus lesion in the follow-up period of 20 years before and after surgical resection of the orbital lesions. We also reviewed 20 patients with orbital myxomas in the literature to know their clinical features.3-22
Case Report
A 41-year-old woman noticed upper eyelid swelling on the right side. At the initial visit, she showed a palpable mass at the superonasal edge of the orbital bone. She did not have medication and no past history of any disease. The best-corrected visual acuity in decimals was 1.5 in both eyes, and the intraocular pressure was 16 mm Hg in both eyes. The both eyes had nothing particular to note, and the eye movement showed no limitation. Magnetic resonance imaging demonstrated a lobulated fluid-containing tubular mass that extended from the posterior to the anterior part of the orbit along the medial orbital wall, nasal to the eyeball (Figure 1A). The contrast enhancement of the tubular mass with gadolinium-DTPA (diethylenetriamine pentaacetic acid) was minimal, indicative of less vascular tissue. The radiographic diagnosis at that time was suspicious of orbital lymphangioma with minimal blood vessel components.

Magnetic resonance imaging. T2-weighted axial image at the age of 41 years at the initial visit (A), showing lobulated fluid-containing mass with probable connection with ethmoid sinus (arrow). T2-wighted axial images with fat suppression by short-T1 inversion recovery, at the age of 48 years (B) and 49 years (C), and (D) just before surgery, showing evident connection with ethmoid sinus (arrows in (B) and (C)) and possible connection posteriorly with sphenoid sinus (large arrow in (C)).
She was followed once a year for 8 years (Figure 1B) until the age of 49 years when she decided to undergo surgical resection because of the enlargement of the mass (Figure 1C and D). The mass was approached from the 10-mm wide skin incision of the upper eyelid on the nasal side, and the resection was planned to be limited to the anterior part of the mass in the safe manner. The lobulated large mass (Figure 2A) was resected, and pathology showed sparsely distributed spindle cells (Figure 2B and C), positive for CD34 (Figure 2E), in alcian blue-positive mucous substances (Figure 2D), indicative of myxoma. She showed no postoperative complication such as diplopia or visual acuity reduction. Postoperative magnetic resonance imaging showed residual lobulated tubular mass along the optic nerve on the medial side and superior to the eyeball (Figure 3A-C). The residual mass showed stable structure for the 12 years until the age of 61 years at the latest follow-up (Figure 3D-F). The connection of the residual orbital lesions with the ethmoid sinus lesion became more evident in the follow-up (Figure 3A and D). She maintained the best-corrected visual acuity of 1.5 in both eyes and had no signs or symptoms such as diplopia and proptosis.

Macroscopic view of extirpated orbital lobulated mass before formaldehyde fixation (A). Microscopic images of the mass in hematoxylin-eosin stain ((B) in low magnification, (C) in high magnification), showing sparse cells in amorphous substance. The amorphous substance is stained positive with alcian blue (D), indicative of mucous substance while cells are positive for CD34 (E). Scale bar = 1000 µm in (B) and 200 µm in (C)-(E).
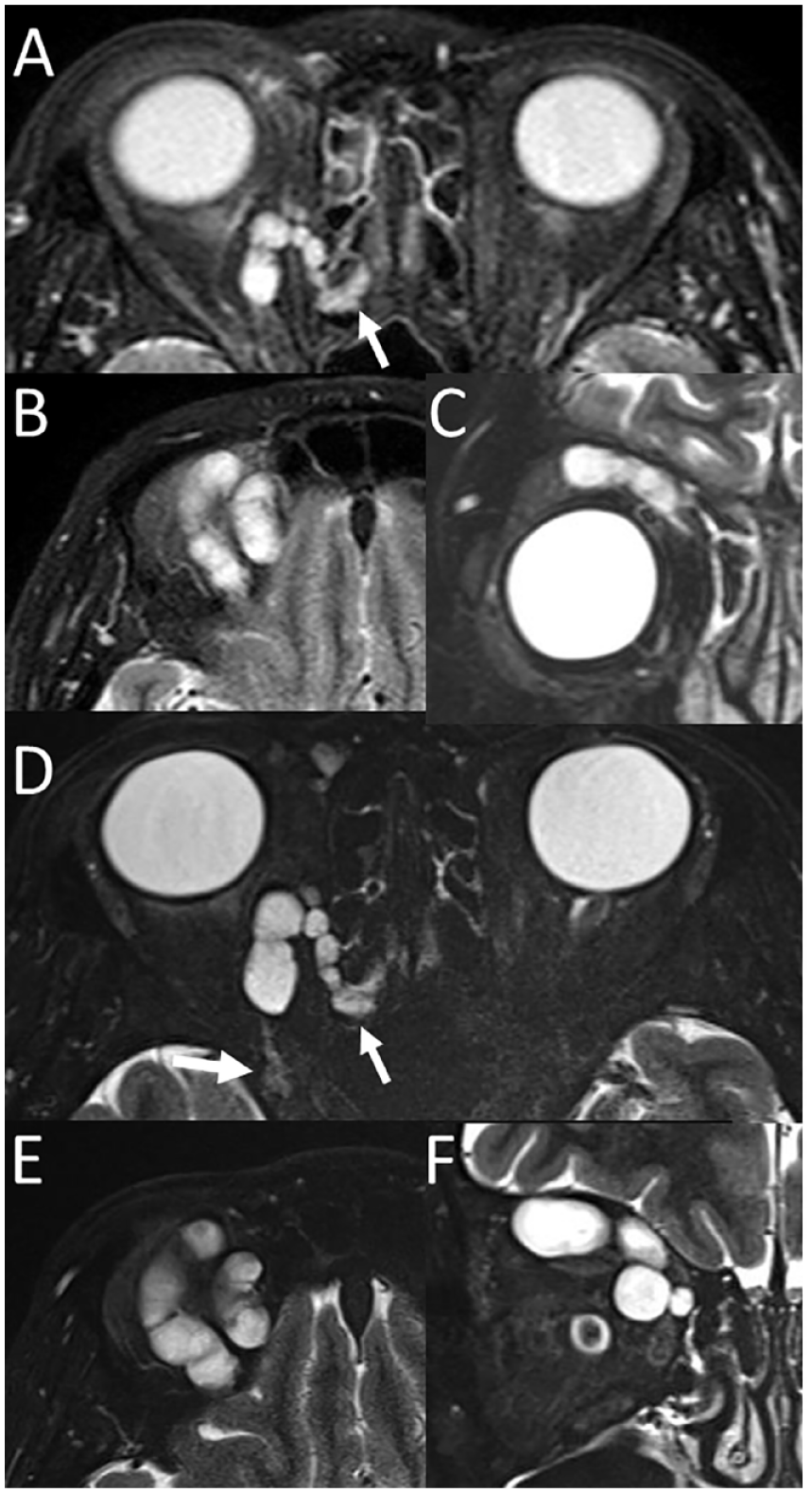
Magnetic resonance imaging. T2-wighted axial (A), (B), and coronal (C) images with fat suppression by short-T1 inversion recovery 3 months after the surgery at the age of 49 years. T2-wighted axial (D), (E), and coronal (F) images with fat suppression by short-T1 inversion recovery at the age of 60 years, 11 years after the surgery. Note connection of the remaining lobulated mass with ethmoid sinus (arrows in (A) and (D)) and possible connection posteriorly with sphenoid sinus (large arrow in D).
Discussion
The present patient was followed in the total of 20 years both before and after the surgical resection. At the initial visit, the clinical diagnosis made by a radiologist was lymphangioma, based on cystic and tubular structure with fluid in magnetic resonance imaging.41,42 As the orbital mass lesion appeared to be benign, a recommended clinical choice was simple observation as far as the mass lesion would not show compressive neuropathies such as vision reduction caused by optic nerve compression and diplopia caused by the compression of eye movement muscles and nerves. In the case of intervention for orbital lymphangioma, clinical choices would be sclerotherapy and surgical extirpation. We did not recommend the patient to undergo sclerotherapy as the sclerotherapy around the eye could have a risk for developing central retinal artery occlusion, leading to the blindness. 43
As described in the case report, the extirpation was planned with the emphasis on surgical safety so as not to damage the optic nerve and extraocular muscles. In the surgery, the tubular structured mass did not show marked adhesion with the surrounding tissues and could be easily pulled out as a lump. Myxoma, or more precisely, intramuscular myxoma, was diagnosed pathologically based on CD34-positive neoplastic cells that were found in a typical feature by hematoxylin-eosin stain. Only after the surgery, it became evident by magnetic resonance imaging that residual parts of the tumor were present mainly in the posterior and upper part of the orbit. In the follow-up, the connection of the residual orbital myxoma lesion to the ethmoid sinus lesion became apparent in the lapse of time. The faint connection of the orbital myxoma to the sphenoid sinus was also evident. These facts suggest that the orbital myxoma would have origin in the paranasal sinuses, mainly the ethmoid sinus.
To analyze similar cases, PubMed and Google Scholar were searched for key words: “myxoma,” “orbital,” “eyelid,” “conjunctiva,” and “ocular adnexa.” We also reviewed the Japanese literature with the same key words to detect no relevant references in the bibliographic database of medical literature in Japanese (Igaku Chuo Zasshi, Ichushi-Web), published by the Japan Medical Abstracts Society (JAMAS, Tokyo, Japan). Old literature was collected from references cited in the articles identified during the literature search. A sufficient description was found in 20 patients with orbital myxoma (Table 1).3,4,6-22
Review of 21 Patients With Orbital Myxoma, Including the Present Patient.
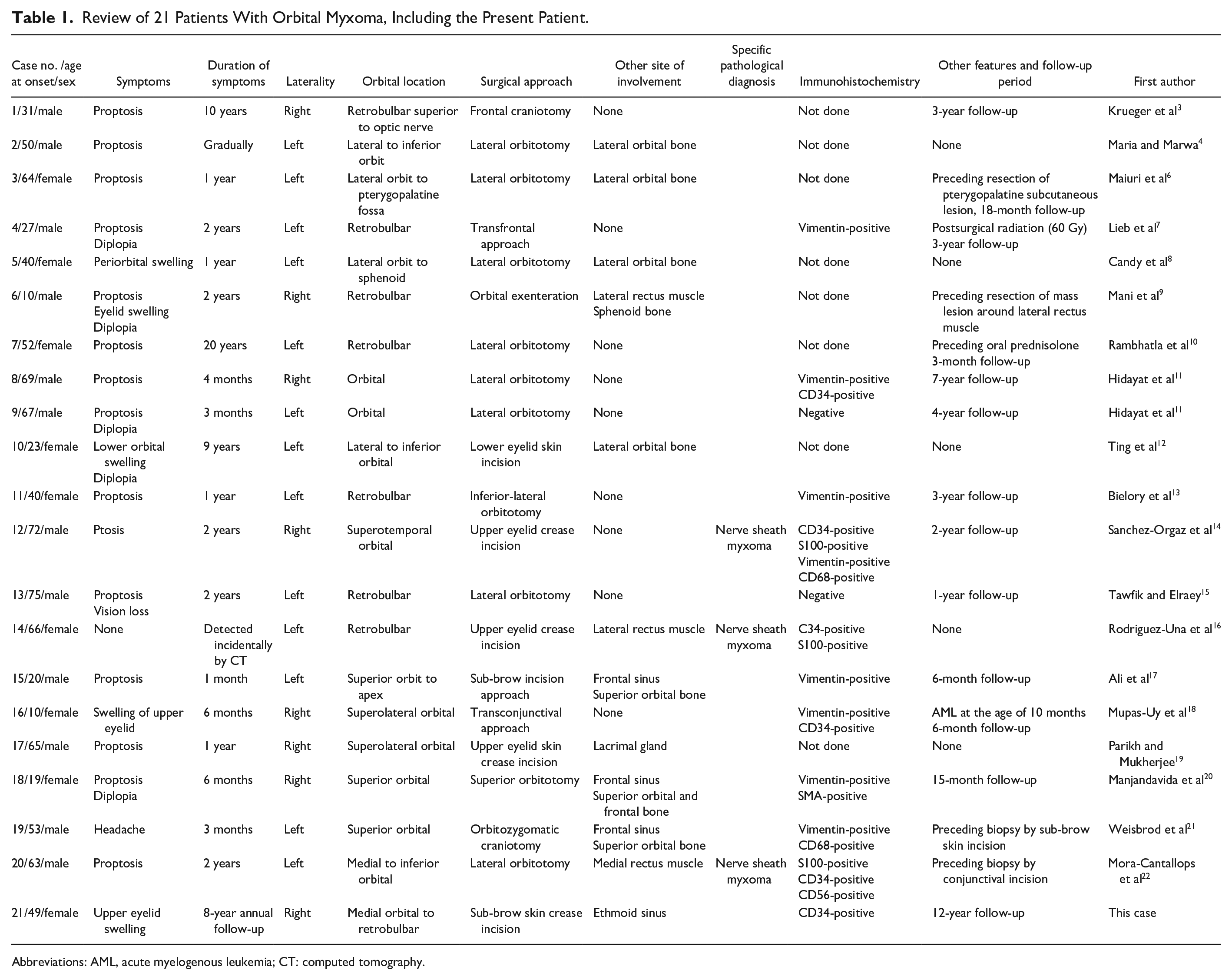
Abbreviations: AML, acute myelogenous leukemia; CT: computed tomography.
As summarized in Table 1, 21 patients, including the present patient, were 12 males and 9 females with the age at the initial presentation ranging from 10 to 75 years (median, 50 years). The initial symptoms were proptosis in 14 patients, eyelid swelling in 5, diplopia in 5, blepharoptosis in 1, headache in 1, and visual loss in 1 (duplicated symptoms in some patients). Orbital myxoma was on the right side in 8 patients and on the left side in 13 patients. Roughly classified locations in the orbit were retrobulbar in 8 patients, on the lateral side of the orbit in 4, on the superior side in 6, on the medial side in 1 (case 21, this patient), and in the orbit with no specific description in 2. Specific tissues in the orbit which were directly involved with myxoma were the lacrimal gland in 1 patient, lateral orbital bone in 4, superior orbital bone in 3, extraocular muscles in 3 (lateral rectus muscle in 2 and medial rectus muscle in 1), and ethmoid sinus (medial orbital bone) in 1 (case 21, this patient). Surgical approaches were lateral orbitotomy in 9, frontal (cranial) orbitotomy in 3, eyelid skin incision in 6, conjunctival incision in 1, orbitozygomatic craniotomy in 1, and orbital exenteration in 1. The preceding resection was done in 2 patients, preceding biopsy was done in 2, and postoperative radiation was done in 1. In pathological examinations, immunohistochemistry was not done in 8 patients, done but all negative in 2, and positive in 11 patients: vimentin was positive in 8, CD34-positive in 6, S100-positive in 3, CD68-positive in 2, CD56-positive in 1, and SMA (smooth muscle actin)-positive in 1 (duplicated positiveness in some patients). Based on the positive S100 staining, nerve sheath myxoma was diagnosed in 3 patients.
The reason why myxoma is predominantly observed in the heart and the head would be its ontogenetic relation with neural crest cells.44,45 Myxoma is considered as a benign tumor which would arise from the remnant primordial tissue. In the head, neural crest cells play a role in the formation of cranial bones and extraocular muscles.46,47 It is interesting to have clinical evidence in this review that myxoma had the involvement with orbital bones and extraocular muscles in some patients. Furthermore, myxomas with spotty skin pigmentation have been described in association with endocrine and neural crest–derived tumors that are known as Carney complex. 48 These lines of clinical evidence, indeed, support that myxoma might have its origin in neural crest–derived cells.
In conclusion, myxoma should be considered in the list of differential diagnosis for cystic and tubular structured tumors in the orbit. As the myxoma is a benign tumor, the decision of its extirpation would be based on the symptomatic and imaging evidence that the tumor would compress other tissues in the orbit such as eyeballs, optic nerve, and extraocular muscles. Partial extirpation of the tumor would be allowed as a surgical procedure to avoid a risk for hurting important tissues such as the optic nerve. Long-term annual observation for 12 years in this patient after the partial extirpation did show that the residual lesions of myxoma in the orbit grew at an extremely slow speed. Additional surgical intervention or other modalities of therapy such as radiation would not be required from the viewpoint of slow growth.
Footnotes
Author Contributions
T.M., as an ophthalmologist, followed the patient, did the surgery, and wrote the manuscript. T.T., as a pathologist, made the pathological diagnosis. All authors approved the final version of the manuscript.
Data availability
Data are available upon reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics committee review was not applicable due to the case report design, based on the Ethical Guidelines for Medical and Health Research Involving Human Subjects, issued by the Government of Japan.
Informed Consent
Verbal informed consent was obtained from the patient for her anonymized information to be published in this article.