
Abstract
Duodenal penetration is a late complication associated with the placement of inferior vena cava (IVC) filters. In this case report, we are presenting a case of asymptomatic duodenal penetration by IVC filter that was managed conservatively.
Keywords
Introduction
Duodenal penetration is a late complication associated with the placement of inferior vena cava (IVC) filters. Inferior vena cava filters are often used in patients with venous thromboembolic disease (VTE) with an absolute contraindication to anticoagulation, complications of anticoagulation resulting in cessation of therapy, or failure of anticoagulation. Although the placement of these filters are generally considered safe, there have been reports of complications such as filter migration, filter fracture, and penetration into adjacent organs, including the duodenum. In this case report, we are presenting a case of asymptomatic duodenal penetration by IVC filter that was managed conservatively.
Case Description
A 79-year-old male with prior history of recurrent deep venous thrombosis (DVT) and pulmonary embolism (PE) status post retrievable (Celect) IVC filter placement, benign prostate hypertrophy, urethral stricture status post chronic suprapubic catheter placement, and visual impairment secondary to glaucoma presented with suprapubic fullness for a few days. He denied nausea, vomiting, constipation, diarrhea, melena, hematochezia, and unintentional weight loss.
He was hemodynamically stable. On examination, his abdomen was soft, nontender, bowel sounds positive, suprapubic catheter draining clear urine, and without abdominal hernias. Laboratory data included hemoglobin 15.4 g/dL, white blood cell count 8.9 × 109/L, platelet 205 × 109/L, creatinine 1.1 mg/dL, and urinalysis without markers of infection. He underwent computed tomography (CT) of the abdomen and pelvis for evaluation of his symptom, and duodenal penetration by the IVC filter strut was identified (Figures 1 and 2). The study was otherwise unremarkable.

CT abdomen and pelvis sagittal view demonstrating one of the IVC filter struts projecting through the vena cava wall into the duodenum (red arrow).
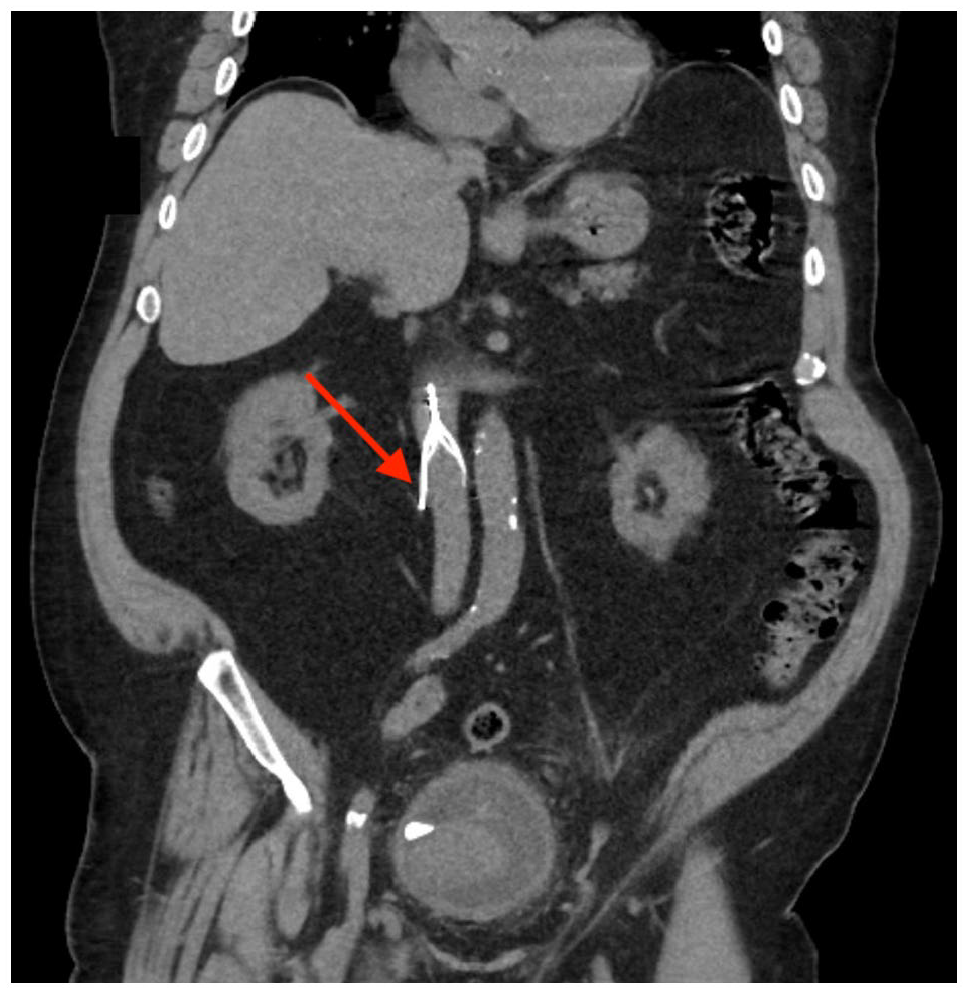
CT abdomen and pelvis coronal view demonstrating one of the IVC filter struts projecting through the vena cava wall into the duodenum (red arrow).
The patient underwent an exchange of the suprapubic catheter, and his symptom resolved. Based on the prompt clinical response, the patient’s presenting symptom is unlikely to be related to the duodenal penetration identified in the CT scan. Our patient underwent retrievable IVC filter placement 6 years prior and was lost to follow-up until the index presentation. He declined endoscopic evaluation of the site of duodenal penetration. After discussion of the treatment options, he opted for conservative management. Two years later, the patient remains asymptomatic and without progressive penetration of the filter in follow-up imaging.
Discussion
The 2 broad categories of IVC filters are permanent (or nonretrievable) and optional (or retrievable). The classic indication for IVC filter placement is in patients with VTE who have an absolute contraindication to anticoagulation. With the advent of retrievable IVC filters, indications have been extended to include iliocaval DVT or large free-floating proximal DVT, difficulty establishing therapeutic anticoagulation, massive PE treated with thrombolysis/thrombectomy, chronic PE treated with thromboendarterectomy, thrombolysis for iliocaval DVT, VTE with limited cardiopulmonary reserve, recurrent PE with filter in place, poor compliance with anticoagulant medications, and high risk of complication with anticoagulation. 1
The removal of retrievable filters can be considered once its indication has resolved. 2 Despite the broader use of retrievable filters, when Ahmed et al 3 analyzed the Medicare Claims Data, the average filter retrieval rate was only 11.6%. Delayed time to retrieval of IVC filters has been linked to increased risk of device-related complications. 4 Gyang et al 5 conducted a study which included 250 patients who underwent IVC filter placement and demonstrated that patients who received follow-up care had significantly higher rate of filter retrieval (93%).
Complications secondary to IVC filters can be classified as insertion-related complications, device failure, and late complications. The late complications are filter thrombosis, fragment embolization, migration, angulation, and penetration of adjacent organs. An analysis of 14,784 patients identified immediate and delayed complications in 1.8% and 3.1% of patients, respectively, during a medium follow-up period of 11 months, but these complications were not associated with increased mortality. 6
The Society of Interventional Radiology defined IVC penetration as extension of the filter elements >3 mm beyond the lumen of the IVC, and most of these patients are asymptomatic. 7 Zhou et al 8 performed a retrospective study of patients who underwent Celect IVC filter placements and the rate of penetration by CT evaluation was 39% within 30 days and 80% within 90 days. Indwelling time >30 months is a risk factor for grade 3 (strut interactions with adjacent organs) penetration of IVC filters. Other risk factors include conical filter, use of retrievable filter, tilting of filter, smaller IVC diameter, underlying malignant disease, and female sex. 9
IVC filter penetrations can affect organs including aorta, duodenum, pancreas, and vertebrae. 10 After a review of the medical literature, we identified 7 publications which included 56 patients with asymptomatic duodenal penetration by IVC filter.11-17 Outcomes were not reported in 46 cases. Among the remaining cases, 8 patients had successful IVC filter removal, 1 patient had failed removal due to an embedded filter tip, and 1 patient received conservative management.
Most patients with asymptomatic duodenal penetrations have undergone removal of the IVC filter as progressive erosion through the IVC wall has been reported in some cases over time. 12 Park et al 14 demonstrated that asymptomatic duodenal penetration can be successfully managed conservatively. Our case reinforces this finding as our patient was managed conservatively and remained asymptomatic in follow-up.
Asymptomatic filter penetrations are commonly diagnosed after CT imaging prior to IVC filter retrieval or for evaluation of symptoms unrelated to the filter penetration. In patients who did not undergo retrieval of the filter, follow-up CT imaging is appropriate to evaluate for progressive erosion through the vena cava. 11 Vena cavagrams are not routinely performed in clinical practice and cannot visualize the outer wall of the IVC, which can lead to false diagnosis of penetration or “pseudopenetration.” 12
In patients presenting with symptoms such as abdominal pain or gastrointestinal bleeding due to duodenal penetration, there is a clear role for endoscopic evaluation. Esophago-gastroduodenoscopy (EGD) has been used in patients with symptomatic duodenal penetration for direct visualization, displacement of the filter tip embedded in the duodenal wall, and for clipping of the penetration site during operative removal of IVC filter.18-20 In patients with asymptomatic duodenal penetration, EGD can be considered if filter removal is being considered. 14
Conclusions
High rates of filter penetration with involvement of adjacent organs are reported in patients with prolonged indwelling time. We recommend implementation of institutional IVC filter registry with aggressive follow-up protocol to increase the retrieval rates and prevent filter penetration. Currently, there are no guidelines for the management of patients with asymptomatic duodenal penetration by IVC filter. Hence, these patients will benefit from a multidisciplinary approach. Our case highlights that conservative management of asymptomatic duodenal penetration can be considered after multidisciplinary discussion in the absence of progressive filter penetration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case studies.
Informed Consent
Verbal informed consent was obtained from the patient for the anonymized information to be published in this article.
Prior Presentation of Abstract Statement
This case was presented as a poster at the American College of Gastroenterology (ACG) 2022 Annual Scientific Meeting at Charlotte, North Carolina, in October 2022.