
Abstract
We present the case of a 30-year-old man with no prior medical history who presented to the hospital with a myriad of symptoms such as shortness of breath, generalized weakness, lower limb weakness, and urinary retention. He was recently diagnosed with “disseminated coccidioidomycosis” by an outside provider on an outpatient basis and started on fluconazole orally. However, due to a lack of improvement and significant symptoms, he was sent to the hospital to initiate liposomal amphotericin B treatment. After a comprehensive workup, an alternative diagnosis was suspected and eventually confirmed as metastatic germ cell carcinoma. Due to the vast dissemination and his poor functional status despite chemotherapy initiation, the patient elected for palliative care and expired shortly after at hospice. This case demonstrates the similarity of clinical findings between disseminated infections and malignancies.
Introduction
Coccidioidomycosis is a common infection in the southwestern United States. It causes a wide range of presentations ranging from asymptomatic to dissemination. Although it usually affects the lungs, it can spread to other organs like skin, bone, joints, or central nervous system. 1
It is important to include other differential diagnoses with similar symptoms and appearance on imaging when clinical suspicion arises. On imaging, coccidioidal infection can mimic other diseases such as malignancies. For instance, it might appear as multiple nodular opacities mimicking lung metastasis or dissemination to bones, particularly to the axial bones, resembling bone metastasis.
Case Presentation
We report a case of a 30-year-old Hispanic man with no known medical history who presented to the emergency department complaining of a 2-week history of shortness of breath, chest pain on deep inspiration, generalized weakness, and dry cough. The patient also endorsed lower back pain radiating to both legs with bilateral lower extremity numbness and tingling associated with bowel and urinary retention for the past 2 months. He was following up with his outside providers who were treating his symptoms as a manifestation of disseminated coccidioidomycosis with fluconazole. He was referred to our institution to start liposomal amphotericin B due to the worsening of his disease.1,2
Upon presentation, vital signs were significant for tachycardia with a heart rate of 128 beats per minute and tachypnea with a respiratory rate of 24 breaths per minute. Physical examination revealed decreased breath sounds on the right side as well as decreased sensation in both buttocks, lateral thighs, calves, and penis. A solitary enlarged tender lymph node with a size of 3 × 3 cm was also noted on the anterior right side of the neck.
Laboratory studies were remarkable for leukocytosis, anemia, thrombocytosis, elevated calcium, C-reactive protein, and erythrocyte-sedimentation rate (Table 1).
Basic Metabolic Panel, Complete Blood Count, and Inflammatory Markers.

Abbreviation: WBC, white blood cells.
Coccidioidomycosis serology was not consistent with the clinical picture of disseminated disease, with weakly reactive immunoglobulin G (IgG) and complement fixation <1:2 (Table 2), which may indicate a previous infection due to living in an endemic area. Therefore, initiation of liposomal amphotericin b was held until further workup. A chest x-ray showed moderate right pleural effusion and left upper lobe nodular opacities [Figure 1] which was confirmed by a chest computed tomography without contrast demonstrating large confluent right perihilar mass-like consolidations, numerous bilateral solid nodules, and moderate right pleural effusion (Figure 2) in addition to widespread sclerotic and mixed sclerotic/lytic lesions throughout the axial and appendicular skeleton (Figure 3). Thoracentesis of the right pleural effusion revealed a hemorrhagic, exudative fluid (Table 2).
Coccidioidomycosis Serology and Pleural Fluid Analysis Obtained From Thoracentesis.


Chest x-ray showing moderate right pleural effusion (blue arrow) and left upper lobe nodular opacities (red arrow).

Axial view computed tomography of the chest showing pleural effusion (blue arrow) and multiple bilateral solid nodules (red arrows).

Sagittal view computed tomography of the spine showing sclerotic (blue arrow) and mixed sclerotic/lytic (red arrow) lesions in the thoracic vertebrae.
The spinal magnetic resonance imaging with and without contrast demonstrated abnormal heterogeneous marrow signal and extensive osseous infiltration on multiple levels of the spine with expansile bony retropulsion mainly at the level of T6 causing spinal stenosis (Figure 4).

Sagittal view magnetic resonance imaging showing spinal cord compression at levels T9, 10, and 11 (blue arrows).
Due to the above workup, an alternative diagnosis of malignancy was considered. Given the patient’s age and the sclerotic appearance of the bony masses on imaging, a testicular malignancy was suspected.
However, ultrasound of the scrotum was unremarkable without any testicular or epididymal masses.
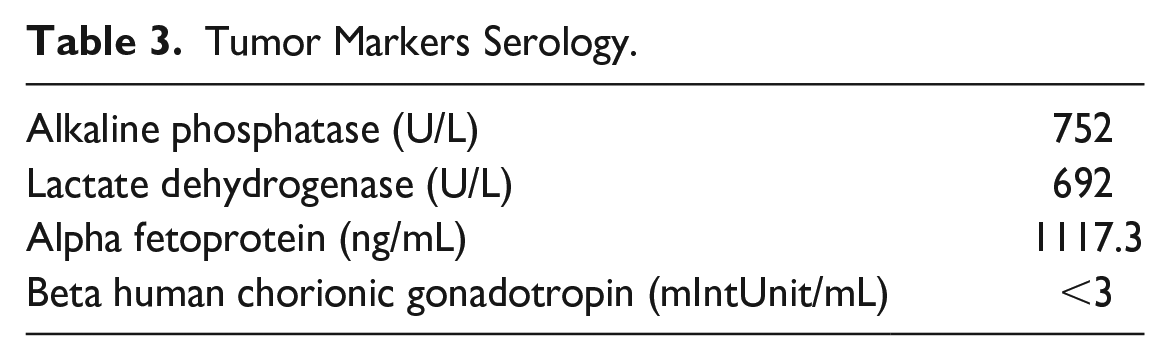
Laboratory studies of alkaline phosphatase (ALP), lactate dehydrogenase (LDH), alpha fetoprotein (AFP), and beta human chorionic gonadotropin (Beta hCG) showed elevated ALP, LDH, and AFP (Table 3).
Tumor Markers Serology.
A cervical lymph node and left transpedicular L1 vertebral body bone biopsy were performed. Histopathology of the lymph node was negative for fungal elements and showed high-grade germ cell neoplasm. Immunohistochemical stains revealed strong positivity of cytokeratin AE1/AE3 and SALL4, consistent with either an embryonal carcinoma or a yolk sac tumor. 3 The L1 vertebral bone biopsy demonstrated osteoblastic bone formation (Figure 5).

(A) Hematoxylin and eosin stain (lymph node biopsy) showing malignant cells (20× magnification). (B) Pancytokeratin stain (lymph node biopsy) showing stained malignant cells (20× magnification). (C) SALL4 stain (lymph node biopsy) showing stained malignant cells (20× magnification). (D) Hematoxylin and eosin stain (L1 vertebral body bone biopsy) showing new bone formation (osteoblastic).
A diagnosis of extragonadal non-seminoma germ cell tumor with metastases was made and the patient was started on a chemotherapy regimen of cisplatin, etoposide, and bleomycin. The patient underwent 4 of 5 days of the first cycle of chemotherapy, but chemotherapy was stopped after the patient elected for palliative care. The patient passed away shortly after.
Discussion
Coccidioidomycosis is a fungal infection caused by the species Coccidioides that is prevalent in the southwestern United States and northern Mexico. The majority of cases recorded in the United States are in Arizona and California.
Coccidioidomycosis has a wide range of presentations from asymptomatic to disseminated, life-threatening disease. It can disseminate to the bone, skin, central nervous system, and many other organs. Along with symptoms associated with the site of dissemination, it has several systemic manifestations such as fever, night sweats, fatigue, and weight loss, which can often mimic noninfectious systemic diseases such as autoimmune disorders and malignancies. Lymph node and osseous dissemination in particular are clinically difficult to distinguish from malignancies with metastases.
Germ cell carcinoma usually presents as a painless testicular mass. It most commonly metastasizes to supraclavicular lymph nodes, lungs, bones, and the central or peripheral nervous system. This can present with findings of a neck mass, respiratory symptoms such as cough or dyspnea, diffuse bone pain, or neurological deficits. Extragonadal germ cell tumors can occur in multiple organs, including the pineal gland, the mediastinum, and the retroperitoneum.
Osseous disseminated coccidioidomycosis and germ cell carcinoma with bone metastases in particular share a very similar presentation. 4 Both diseases present with diffuse bone pain, mass effect on nearby neurological structures, weight loss, and fatigue. The presence of past infection with coccidioidomycosis makes it more enigmatic as the reactivation of infection can occur either spontaneously or triggered by the new diagnosis of malignancy due to its impact on the immune system.
In this case, the patient was likely diagnosed with coccidioidomycosis in the past, as evidenced by the positive IgG titers. Starting fluconazole therapy was probably the correct decision at the time of diagnosis when IgM was presumably positive and the titers were higher. However, the downtrend in complement fixation titers without parallel clinical improvement despite more than 18 months of treatment should alert the physician to an alternate diagnosis other than coccidioidomycosis. Although response to therapy varies from case to case, the discrepancy between titers and clinical symptoms is the trigger warning that should lead to further work up.
Despite the many similarities between both diseases, clues that favor one over the other should be investigated. Although testicular involvement in disseminated coccidioidomycosis was reported in multiple case reports, it remains uncommon and it should raise suspicion of a germ cell carcinoma as a more probable explanation, especially in younger patients. Travel and exposure history is another key element in history-taking that would favor disseminated coccidioidomycosis if the patient has recently visited the endemic area. Coccidioidomycosis serology is another tool that would favor the diagnosis of disseminated coccidioidomycosis particularly with high-complement fixation titers. Histopathology along with microbiology remains the most definitive distinctive test.
Pulmonary manifestation of coccidioidomycosis may present as infiltrations, cavitary lesions, or nodules with or without an associated parapneumonic effusion on chest x-ray. It might also be associated with hilar or mediastinal lymphadenopathy. Although this patient’s chest x-ray shows pleural effusion and a nodular opacity, the extent of the lesions points toward a more aggressive pathology.
Biopsy of an extrapulmonary lesion with histopathologic identification or fungal isolation is usually necessary for diagnosis of disseminated coccidioidomycosis. Reli-ance solely on positive titers with a clinical picture of dissemination yields many false-positive cases that are misclassified with the disease and treated inappropriately with antifungals.
Conclusion
Disseminated coccidioidomycosis and germ cell carcinoma could share a very similar presentation. High suspicion of one should rise when considering the diagnosis of the other.
Footnotes
Acknowledgements
We acknowledge the role of all the co-authors in the making, editing, and finalizing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Prior Presentation of Abstract Statement
This abstract was presented as a poster at the American Federation of Medical Research’s Western Conference, Carmel, CA, in January 2023. It was also chosen as a finalist abstract in the American College of Physicians (ACP) Southern California Meeting in San Diego, CA, in October 2022.
Ethical Approval
Ethical approval to report this case was obtained from the Kern Medical Institutional Review Board (IRB 21118).
Informed Consent
Written informed consent was obtained from the patient for their anonymized information and photography to be published in this article.