
Abstract
A 63-year-old woman, with 11-year history of breast cancer, showed bilateral lacrimal gland enlargement on magnetic resonance imaging. Gallium-67 scintigraphy, as the standard at that time in 2004, demonstrated abnormally high uptake only in bilateral lacrimal glands. The lacrimal glands were extirpated and the pathological diagnosis was mantle cell lymphoma (MCL). She underwent bilateral orbital radiation, based on no uptake of gallium-67 in other sites of the body. In a month, bone marrow biopsy revealed the infiltration with MCL, positive for cyclin D1. She showed hepatic lymphadenopathy and splenomegaly, and so received 2 cycles of alternating Hyper-CVAD therapy and high-dose methotrexate with cytarabine, combined with rituximab, in 2 months, leading to complete remission. She underwent autologous peripheral blood stem cell transplantation and was well until the age of 68 years when she showed a recurrent intratracheal submucosal lesion of lymphoma and underwent one course of reduced-dose CHOP combined with rituximab. Next year, the left rib resection revealed the metastasis of breast adenocarcinoma, leading to daily oral letrozole. Further 2 years later, computed tomographic scan demonstrated multiple submucosal nodular lesions in the trachea and bronchi, together with cervical and supraclavicular lymphadenopathy, and intratracheal lesion biopsy and bone marrow biopsy proved the involvement with MCL. She underwent 2 courses of bendamustine and rituximab, resulting in complete remission but died of metastatic breast cancer at the age of 74 years. Clinical features in 48 previous cases with ocular adnexal MCL in the literature were summarized in this study.
Keywords
Background
Lymphoma is the most frequent malignancy encountered in the field of ophthalmology where malignant diseases are basically rare. Two major clinical entities of lymphoma in the ophthalmic presentation are intraocular lymphoma1-4 and ocular adnexal lymphoma.5-8 The intraocular lymphoma is classified into primary and secondary intraocular lymphoma. The primary intraocular lymphoma develops in association with primary central nervous system lymphoma1-4 while the secondary intraocular lymphoma is caused by infiltration of lymphoma which initially occurs at the other sites of the body.9-11 The clinical manifestations of the intraocular lymphomas are vitreous opacity and retinal infiltrates and must be differentiated from inflammatory presentation of uveitis.12,13
The ocular adnexa is the anatomical term to indicate all tissues which support the eyeball in the orbit such as lacrimal glands and sacs, eyelids, conjunctiva, extraocular muscles, and the soft tissue. The ocular adnexa is the site not only for lymphoma but also for inflammatory diseases such as IgG4-related disease,14-17 sarcoidosis, 18 and other inflammatory entities.19,20 In the ocular adnexa, the lacrimal glands and conjunctiva21-24 are 2 major sites for both lymphoma and inflammatory diseases. Inflammatory diseases in these sites might play a role in predisposing the development of lymphoma.17,18,20
Lymphoma has been classified into different histopathological types which are associated with different clinical prognosis.25-27 Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue, so-called MALT lymphoma, is the most frequent diagnosis in the ocular adnexal lymphoma and has favorable outcome based on its slow progression and less infiltration to other sites of the body. The other types of lymphoma such as mantle cell lymphoma (MCL)28-32 are relatively rare, and their prognosis is not so favorable compared with MALT lymphoma. In this study, we presented a patient with primary MCL in bilateral lacrimal glands who, after all, underwent autologous peripheral blood hematopoietic stem cell transplantation in the background of breast cancer. In the end of the long-term follow-up, the relapse of MCL occurred in parallel with the metastatic lesion of breast cancer. We also summarized 48 patients with MCL in the literature who presented with ocular adnexal lesions in order to elucidate their clinical features.33-77
Case Report
A 63-year-old woman noticed upper eyelid swelling on the right side half a year previously and visited a local eye doctor. She underwent laser peripheral iridotomy in both eyes for shallow anterior chamber and was referred to Okayama University Hospital. At that time, she did not take any medication. In the past history, she had undergone left mastectomy for breast ductal adenocarcinoma at 52 years old and discontinued postoperative oral medication for breast cancer due to allergic skin reaction.
At the initial visit, the best-corrected visual acuity in decimals was 1.5 in both eyes and the intraocular pressure was 12 mm Hg in both eyes. She had nothing particular in both eyes except for peripheral iridotomy in the superonasal quadrant. The lacrimal glands on both sides were palpable at the orbital bony edge. Gallium-67 scintigraphy showed abnormally high uptake only in bilateral lacrimal glands (Figure 1A) and magnetic resonance imaging demonstrated the enlargement of bilateral lacrimal glands (Figure 1B and C). She underwent lacrimal gland extirpation on both sides in August 2004 and the pathological diagnosis was MCL, based on the infiltration with small monotonous cells (Figure 2A) which were positive for cyclin D1 (Figure 2B), CD5, CD20 (Figure 2D), and CD79a, but negative for CD3. Ki-67 labeling index was less than 1 % (Figure 2C).

Gallium-67 scintigraphy (A), showing high uptake in bilateral lacrimal glands, and magnetic resonance imaging, showing bilateral lacrimal gland masses in axial (B) and coronal section (C) at the initial visit at the age of 63 years.
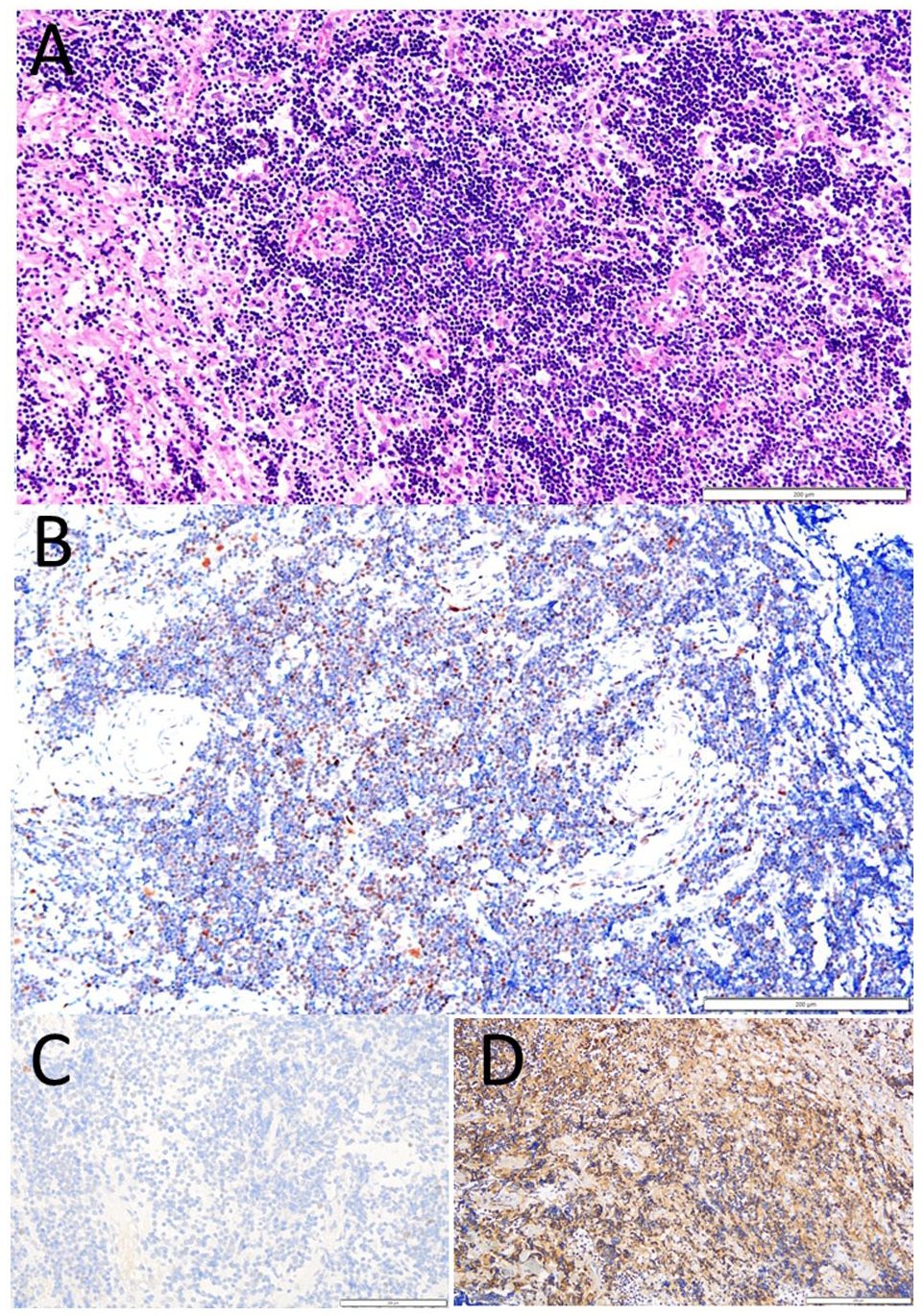
Right lacrimal gland extirpated at the age of 63 years. Infiltration with monotonous cells (A, hematoxylin-eosin), positive for cyclin D1 (B) and CD20 (D). Ki-67 labeling index was less than 1 % (C). Cyclin D1 was re-stained in 2021 with anti-cyclin D1 antibody (Abcam SP4, rabbit monoclonal, ×150 dilution). Ki-67 was re-stained in 2023 (NCL-Ki67p, Leica Biosystems, rabbit polyclonal, ×500 dilution). Scale bar = 200 µm.
Based on no uptake of gallium-67 in other sites of the body, she underwent radiation at the total dose of 40 Gy (2 Gy × 20 fractions) on both sides of the orbit in 4 weeks. After the completion of radiation, bone marrow biopsy revealed the infiltration with MCL (Figure 3A), positive for cyclin D1 (Figure 3B). She showed systemic superficial lymphadenopathy, splenomegaly, and hepatic portal lymphadenopathy up to the diameter of 6 cm and was designated as Stage IV. Serum lactate dehydrogenase was 268 IU/L (laboratory upper limit of the normal range: 220 IU/L), serum soluble interleukin-2 receptor was elevated to 1860 U/L, and white blood cell counts were 5.09 × 103/µL. There was no involvement in the liver, bilateral lung fields, or mediastinal lymph nodes. Her performance status was 1. She underwent 2 cycles of alternating Hyper-CVAD therapy (cyclophosphamide 500 mg × 2, doxorubicin 70 mg, vincristine 2 mg, and dexamethasone 40 mg) and HD-MA therapy (methotrexate 300 mg and 1200 mg, cytarabine 1400 mg × 2) in 2 months, leading to complete remission. Rituximab every 3 weeks, 8 times in total, was combined from the beginning of chemotherapy until the autologous peripheral blood stem cell transplantation. Bone marrow biopsy confirmed no involvement, and peripheral blood stem cells were collected twice after HD-VP therapy (etoposide 700 mg) and HD-MA therapy. In myeloablative conditioning with LEED therapy (cyclophosphamide 3000 mg, etoposide 700 mg, melphalan 200 mg, and dexamethasone 40 mg), she underwent autologous peripheral blood stem cell transplantation successfully in May 2005. Three years later at the age of 67 years, she underwent cataract surgery in both eyes for radiation cataract.

Bone marrow biopsy at the age of 63 years. Infiltration with monotonous cells (A, hematoxylin-eosin), positive for cyclin D1 (B). Cyclin D1 was re-stained in 2021 with anti-cyclin D1 antibody (Abcam SP4, rabbit monoclonal, ×150 dilution). Scale bar = 200 µm.
She was well until the age of 68 years in May 2009 when she developed a recurrent intratracheal submucosal lesion of lymphoma and underwent one course of reduced-dose CHOP, combined with 4 courses of rituximab, nearing to complete remission. At the age of 69 years in April 2010, the left rib resection revealed the metastasis of breast adenocarcinoma, leading to the start of oral letrozole 2.5 mg daily. Two years later in July 2012, computed tomographic scan demonstrated multiple submucosal nodular lesions in the trachea and bilateral bronchi, together with bilateral cervical and supraclavicular lymphadenopathy, and intratracheal lesion biopsy and bone marrow biopsy proved the involvement with mantle cells lymphoma. She underwent 2 courses of bendamustine (60 mg/m2 on Day 1 and 2) and rituximab (375 mg/m2), resulting in complete remission. In April 2014, she had no medication and visited an eye doctor with no abnormal finding. One year later in April 2015, she died of metastatic breast cancer at the age of 74 years.
Discussion
A hallmark in the diagnosis of MCL is the overexpression of cyclin D1 in the nuclei of monotonous cells with B-cell lineage. In the present patient, cyclin D1 was re-stained on paraffin sections of the extirpated lacrimal gland and the bone marrow biopsy specimen which have been preserved since the initial presentation in 2004. At that time, fluorodeoxyglucose-positron emission tomography had not yet been introduced and could not be used for the staging of lymphoma as is the current standard. Based on the absence of abnormal uptake in the other sites of the body by gallium-67 scintigraphy, the patient underwent local radiation. However, in the light of MCL as a pathological diagnosis, the bone marrow was examined by biopsy to check the systemic infiltration. Around the same time, the patient developed superficial lymphadenopathy, and computed tomography disclosed hepatic lymphadenopathy in large size as well as splenomegaly.
Retrospectively, the simplified MCL international prognostic index (MIPI) score 78 which was not available at the time before systemic chemotherapy in this patient was calculated as 5 and designated as intermediate: 2 points for the age at 64 years, zero point for the performance status at 1, 2 points for LDH/ULN (laboratory upper limit of the normal) ratio as 268/220 = 1.21, and zero point for white blood cell counts at 5.09 × 103/µL. Therefore, systemic chemotherapy and autologous peripheral blood stem cell transplantation as a therapeutic strategy in this patient would be compatible with the current standard. From the pathological point of view, the lacrimal gland lesion in this patient showed a low Ki-67 index in small monotonous lymphoma cells. The patient presented bone marrow involvement and splenomegaly, and thus, would be diagnosed as small cell variant of MCL which might show indolent course. 79 It should be, however, noted that the relapse did occur in the present patient after the autologous peripheral blood stem cell transplantation. The relapse of MCL was diagnosed by repeat pathological examinations and managed by additional chemotherapy in the time course which was intervened by the pathological confirmation of rib metastasis of breast adenocarcinoma. The patient was healthy until the death of metastatic breast cancer.
To analyze similar cases, we reviewed the Japanese literature with key words, “mantle cell lymphoma,” “lacrimal gland,” “lacrimal sac,” “orbital,” and “ocular adnexa,” in the bibliographic database of medical literature in Japanese (Igaku Chuo Zasshi, Ichushi-Web), published by the Japan Medical Abstracts Society (JAMAS, Tokyo, Japan). Old literature was collected from references cited in the articles identified during the literature search. PubMed and Google Scholar were also searched for the same key words. A sufficient description was found in 48 patients with ocular adnexal MCL (Table 1).33-77
Review of 49 Patients With Ocular Adnexal Mantle Cell Lymphoma, Including the Present Patient.

Abbreviations: Hyper-CVAD, cyclophosphamide, vincristine, doxorubicin, dexamethasone; MTX, methotrexate; VEMP, vincristine, cyclophosphamide, mercaptopurine, prednisolone; R-CVP, rituximab, cyclophosphamide, vincristine, prednisolone; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisolone; AraC, cytarabine; mTHPC, 5,10,15,20-tetra(m-hydroxyphenyl)chlorin; FCR, fludarabine, cyclophosphamide, rituximab; R-GIFOX, rituximab, gemcitabine, ifosfamide, oxaliplatin; R-DHAP, rituximab, dexamethasone, high-dose cytarabine, cisplatin; R-THP-COP, rituximab, pirarubicin, cyclophosphamide, vincristine, prednisolone; CHASER, cyclophosphamide, high-dose cytarabine, dexamethasone, etoposide, rituximab; VR-CAP, bortezomib, rituximab, cyclophosphamide, doxorubicin, prednisolone; R-ICE, rituximab, ifosfamide, carboplatin, etoposide.
The 49 patients, including the present patient, were 33 men and 16 women with the age at the initial ophthalmic presentation ranging from 24 to 84 years (median, 65 years). The bilateral involvement was noted in 26 patients while the unilateral involvement was in 23 patients: 13 on the right side and 10 on the left side. Lacrimal gland MCL was diagnosed in 17 patients, conjunctival lymphoma in 10, and lacrimal sac lymphoma in one while lymphoma in the other regions of the orbit was diagnosed in the remaining 21 patients. Two of these 21 patients with orbital lymphoma showed the involvement of the bilateral optic nerve sheath which caused optic neuropathy. One of the 10 patients with conjunctival lymphoma also showed intraocular involvement which manifested uveitis and choroidal infiltration. The ophthalmic presentation was the initial symptoms at the onset of MCL in 37 patients while the previous diagnosis of MCL had been made in the remaining 12 patients. Most patients developed systemic infiltration except for 6 patients with the description of localized lesions in the ocular adnexa. As for the treatment, most patients underwent systemic chemotherapy and autologous peripheral blood stem cell transplantation was done in 6 patients. Local radiation was done as a sole treatment or additional palliative treatment in 7 patients. The follow-up periods were not described or otherwise short up to 3 years.
Other than the direct involvement of ocular adnexa with MCL as described above, neurological consequences of the central nervous system infiltration have to be considered in making a diagnosis. 80 Indeed, acute bilateral ophthalmoplegia has been reported as an initial manifestation of MCL as the result of central nervous system infiltration. 81 Regarding a new mode of treatment, proton beam therapy has been applied to the residual lesions in the orbit after systemic chemotherapy. 82 In the present patient, the initial lacrimal gland lesions of MCL were locally controlled in a successful manner by radiotherapy. Autologous hematopoietic stem cell transplantation has been established as the standard treatment option in relapsed or newly diagnosed MCL,83,84 as shown in the present review. In conclusion, we described a long-term outcome of 11 years in a patient who underwent autologous peripheral blood stem cell transplantation for the systemic infiltration of bilateral lacrimal gland MCL as an initial presentation. To the best of our knowledge, the follow-up period in this patient is longest in the literature.
Footnotes
Authors’ Note
Data are available upon reasonable request to the corresponding author.
Author Contributions
T.M., as an ophthalmologist, performed surgery, followed the patient, and wrote the manuscript. T.T. and K.N., as pathologists, made pathological diagnoses. K.O., K.F., and N.F., as oncologists, treated the patient. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics committee review was not applicable due to the case report design, based on the Ethical Guidelines for Medical and Health Research Involving Human Subjects, issued by the Government of Japan.
Informed Consent
Verbal informed consent was obtained from the patient for her anonymized information to be published in this article.