
Abstract
Gastric volvulus is a rare medical condition that necessitates a high suspicion index to diagnose. Acute gastric volvulus will often present with nonspecific but severe symptoms of abdominal pain, nausea, vomiting, and in some instances, evidence of organ ischemia. In this case report, we present an 88-year-old woman who was admitted after a mechanical fall. On the third day of hospitalization, she complained of new-onset epigastric pain, nausea, and vomiting. Imaging demonstrated nonobstructed intrathoracic organo-axial gastric volvulus. Given the patient’s significant comorbidities, surgical and endoscopic interventions were deemed high-risk (high risk of anesthesia and gastric perforation, respectively). This report evaluates the role of noninterventional conservative management in high-risk surgical patients with symptomatic acute and acute-on-chronic intrathoracic gastric volvulus. The present case and the current literature review suggest that supportive management may be appropriate to control disease symptoms, although it does not alter the disease’s natural history, progression, and recurrence.
Keywords
Background
We here present a case of chronic gastric volvulus, an extremely rare condition that is primarily seen in adults older than 50 years. It is characterized by the abnormal rotation of the stomach along its horizontal or vertical axis. 1 Gastric volvulus can be either primary (second to gastric ligaments abnormalities) or secondary (second to anatomic abnormalities) other than gastric ligaments (eg, para-esophageal hernia and diaphragmatic hernia).2,3
Case Report
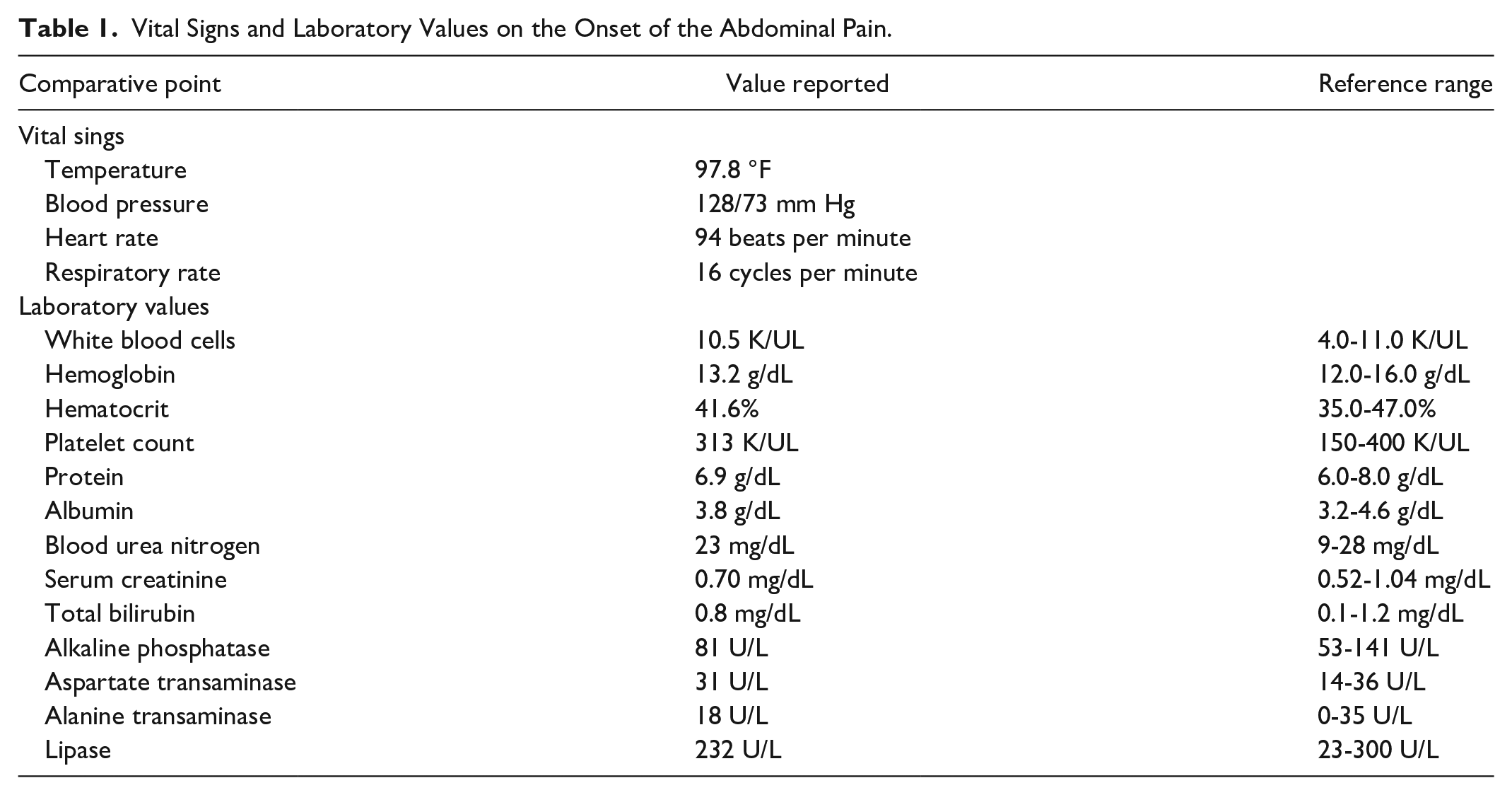
We present an 88-year-old woman with a past medical history of hypertension, hiatal hernia, total abdominal hysterectomy, and dementia complicated by malnutrition and poor oral intake, who was brought to the emergency department for a fall. The patient was found to have no fractures or intracranial hemorrhage and received the appropriate supportive medical treatment. However, on the third day of admission, she reported new onset abdominal pain, nausea, and bilious vomiting. Vital signs were stable, and laboratory workup was unremarkable (Table 1). Computed tomography (CT) scan of the abdomen with contrast showed the stomach to be largely contained within the right hemithorax and rotated along its long axis compatible with an organo-axial volvulus, yet was nondilated nor obstructed, with contrast visualized throughout nondilated loops of small bowel which seem to be chronic in etiology as there were intrathoracic bowel loops on abdominal imaging 6 months prior (Figure 1). Review of previous images noted the presence of the intrathoracic stomach on a CT scan done 12 years prior (Figure 1). Gastroenterology and general surgery evaluated the patient and thought that she was a very high risk for sedation and anesthesia given the history of worsening dementia, her debilitated medical condition, and diminished oral intake with malnutrition. Hence, it was decided that there was no role for endoscopic or surgical intervention to correct the organo-axial volvulus at the present time. Several attempts to place nasogastric tube (NGT) were, however, unsuccessful. The patient was started on total parenteral nutrition under the care of the hospital nutritionists. Over the next 3 days, and with frequent re-orientation and the patient’s family attempting to orally feed her, the patient’s abdominal pain improved, and she was able to tolerate increased oral intake. The patient was discharged to a sub-acute rehab. On evaluation, 1 month later, the patient has had no more abdominal symptoms, continued to have adequate oral intake, with considerable improvement of her mental status and physical capabilities. Four months later, the patient was re-admitted to the hospital for new-onset atrial fibrillation (Afib). The Afib was managed conservatively and subsequently discharged back to her nursing home. Of note, she was alert and oriented during the hospitalization period, had no abdominal complaints, and was able to maintain an oral diet during the hospital stay.
Vital Signs and Laboratory Values on the Onset of the Abdominal Pain.
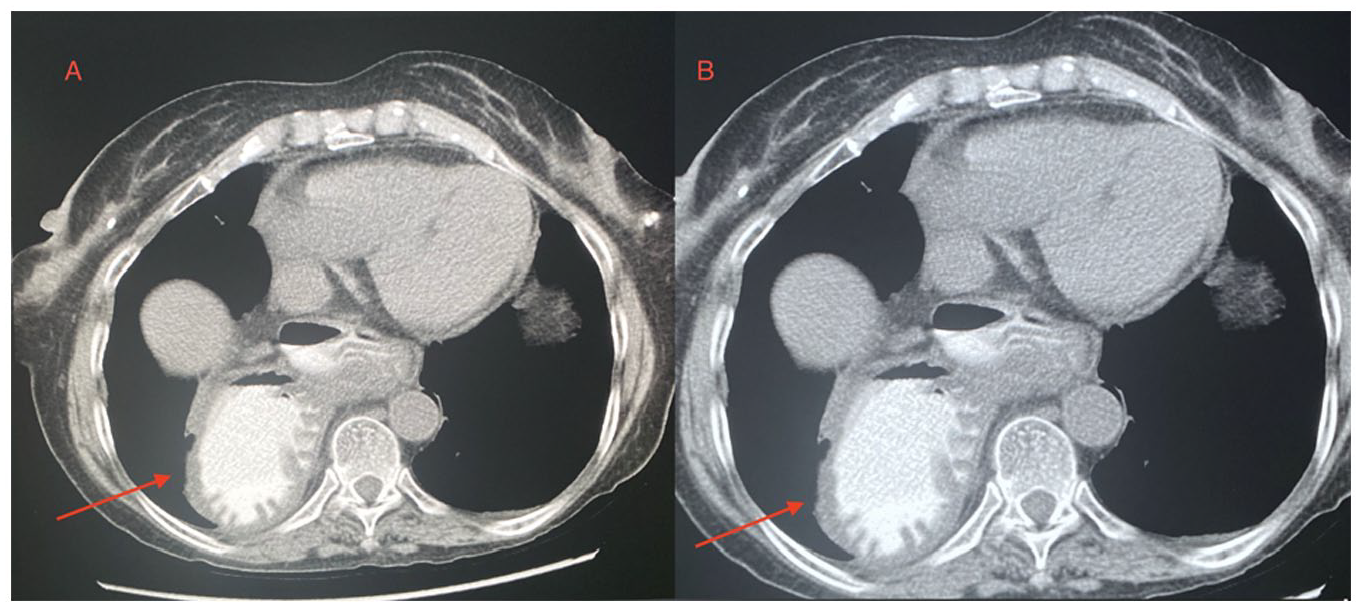
Computed tomography scan of the abdomen (axial view) performed on this admission (on the left (A)) versus 12 years prior (on the right (B)). The arrow points to the intrathoracic gastric volvulus.
Discussion
The diagnosis of gastric volvulus is difficult to make and requires a high index of suspicion. The most common presentation is in an elderly patient with history of gastroesophageal reflux (GERD) and paraesophageal hernia who presents with acute or subacute abdominal pain. 4 Borchardt’s triad (abdominal pain, repetitive vomiting, and failure to pass a nasogastric tube (NGT)) was reported in 70% of acute gastric volvulus cases. 5 On the contrary, chronic gastric volvulus presents with nonspecific symptoms, including mild upper abdominal pain, abdominal bloating, heartburn, nausea, vomiting, difficulty swallowing, early satiety, and rarely bronchobiliary fistula.6,7 Despite presenting with a new onset epigastric pain, nausea, and vomiting, our patient reported a history of similar episodes in the past, which usually subside on their own. Similarly, imaging confirmed an intrathoracic stomach which was noted on a previous CT scan (12 years prior). Therefore, our case report highlights that chronic gastric volvulus may contribute to patients’ intermittent vague upper GI symptoms with a relatively low probability of developing further complications.
Gastric volvulus management typically starts with stabilizing the patient with fluid resuscitation, electrolyte correction, and gastric decompression. Gastric decompression can be done through NGT insertion or, if NGT decompression is unsuccessful (as in our patient), endoscopic decompression. Ideally, endoscopic decompression and/or de-rotation are best performed under anesthesia while the patient is intubated. If endoscopic gastric decompression is unsuccessful, surgical intervention is required.1,8,9 Our patient had a very high medical and anesthetic risk. After a multidisciplinary team discussion that included the patient’s family, the decision was made to proceed with conservative management.
The current literature suggests that once the patient is medically stabilized and gastric decompression has been achieved, definitive treatment is indicated. 2 Open surgical approach, namely, “decompression and de-rotation,” is recommended in unstable patients, with gastric resection reserved in patients demonstrating signs of irreversible gastric ischemia. Stable patients usually undergo laparoscopic gastric reduction and de-rotation (typically through gastropexy (for primary volvulus) or anatomical defect repair (for secondary volvulus; eg, paraesophageal hernia)). Endoscopic de-rotation and percutaneous endoscopic gastrostomy (PEG) tube placement is the first-line treatment for primary gastric volvulus and poor surgical candidates with secondary gastric volvulus10,11 Typically, 2 PEG tubes are placed, 1 placed into the gastric body and the other further distal (as gastric re-rotation may still occur with 1 PEG tube). 12 However, endoscopic gastric fixation using PEG tube has shown variable results, specifically among poor surgical candidates. 13
In this report, we demonstrated that conservative management is, perhaps, a more appropriate approach in patients with chronic gastric volvulus who are poor endoscopic or surgical candidates. Furthermore, our patient’s mental status and ability to tolerate oral diet has improved with adequate supportive measures (frequent re-orientation; meeting needs for nutrition, fluids, and sleep). At this time, we are unable to suggest any causation or correlation. Such findings were previously suggested in the literature, where 1 study reported that none of the 44 patients developed a devastating complication during the 5-and-half-year follow-up period of sole conservative treatment. 6
Most importantly, the available literature suggests several factors to be associated with symptom recurrence, including a longer duration between the initial onset of symptoms and diagnosis, history of previous abdominal surgeries, and presence of peritoneal adhesion(s).6,14,15 One study suggested that almost two-thirds of the patients without anatomical correction experienced recurrent symptoms within the median follow-up period of 16 months. 6 However, this is expected, as symptom recurrence in uncorrected gastric volvulus is an inherent component of the natural history and pathogenesis of such a condition. Hence, we conclude that our patient remains at a high risk given the history of abdominal hysterectomy for a leiomyoma, and thus close monitoring is necessary.
Conclusion
Chronic intrathoracic gastric volvulus is a rare medical condition with nonspecific symptoms making the diagnosis challenging to establish. Our report supports the role of conservative management in patients with chronic gastric volvulus who are poor endoscopic or surgical candidates. Nevertheless, large, randomized control trials are essential to evaluate the role of conservative versus interventional management (both endoscopic and surgical) of gastric volvulus with a long-term follow-up for evaluation of recurrence.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual case.
Informed Consent
Verbal informed consent was obtained from the patient’s power of attorney (the son) for the patient’s anonymized information to be published.