
Abstract
Hepatic adenomas (HAs) are rare but benign neoplasms of the liver which predominantly present as solitary lesions in women of reproductive age. The incidence of HAs has increased dramatically since the introduction of oral contraceptive pills (OCPs) along with the rising incidence of obesity. Discontinuation of OCPs and lifestyle modifications, including weight loss regimens, are considered as conservative treatment options for HAs. Large lesions may result in malignant transformation with a higher propensity for hemorrhage. Importantly, larger lesions that do not respond to conservative management require surgical excision. We report a case of a patient presenting with multiple hepatic lesions that were subsequently confirmed as HAs.
Introduction
Hepatic adenomas (HAs) are benign tumors of the liver of presumable epithelial origin and occur in less than 0.04% of the population. 1 They typically present as solitary lesions and are usually found incidentally. HAs can result in spontaneous hemorrhage in 20% of patients leading to an increased risk of post-liver biopsy hemorrhage. 2 Lesions larger than 5 cm occur in less than 20% of cases. 3 Such large lesions have a higher chance of malignant transformation, rupture, and spontaneous hemorrhage. 2 The incidence of HAs significantly rises with the use of oral contraceptive pills (OCPs) and in patients who are obese. 4
We report an unusual yet significant case of a young obese female on OCPs found to have multiple HAs. Following a liver biopsy, the patient developed bleeding as well as intraparenchymal and subcapsular hematomas which required embolization to control the hemorrhage.
Case Presentation
A 37-year-old female with no significant medical history presented to the emergency department of a local hospital with a 4-week history of right upper quadrant (RUQ) abdominal pain. Her recent gynecological evaluation was unremarkable. Medication history was notable for long-term OCP use and occasional use of nonsteroidal anti-inflammatory drugs. She denied any history of smoking or alcohol use. Her vital signs were stable and physical examination was unremarkable. Her body mass index was 35.6 kg/m2. Initial liver function tests (LFTs) were notable for an aspartate transaminase (AST) of 320 U/L, alanine transaminase (ALT) of 769 U/L, and alkaline phosphatase of 67 U/L. Repeat LFTs after 2 weeks revealed AST of 22 U/L and ALT of 109. Ultrasound of the RUQ abdomen revealed multiple hypoechoic lesions of the liver, with the largest measuring 8 cm in diameter. The gallbladder appeared normal. Computed tomography (CT) of the upper abdomen with oral and intravenous (IV) contrast revealed multiple large liver masses along with scattered and small lesions in both hepatic lobes consistent with the same process (Figure 1). The patient had approximately 5 lesions. These imaging findings were concerning for hepatocellular carcinoma versus metastatic disease versus focal nodular hyperplasia. HA was not considered in the differential diagnoses initially due to presence of multiple lesions. Alpha-fetoprotein level was within normal limits at 1.1. Subsequent liver biopsy revealed that the lesions had pathological findings indicative of HA (Figures 2 and 3). These findings were independently confirmed by 2 pathologists. After the biopsy, the patient developed bleeding into the liver. Repeat CT revealed intraparenchymal and subcapsular hematomas. The patient’s bleeding and general status improved after embolization. OCPs were discontinued and her lesions are regressing. She is still being monitored for resolution of HAs. Surgery is following to evaluate for a potential hepatectomy if HAs do not resolve.
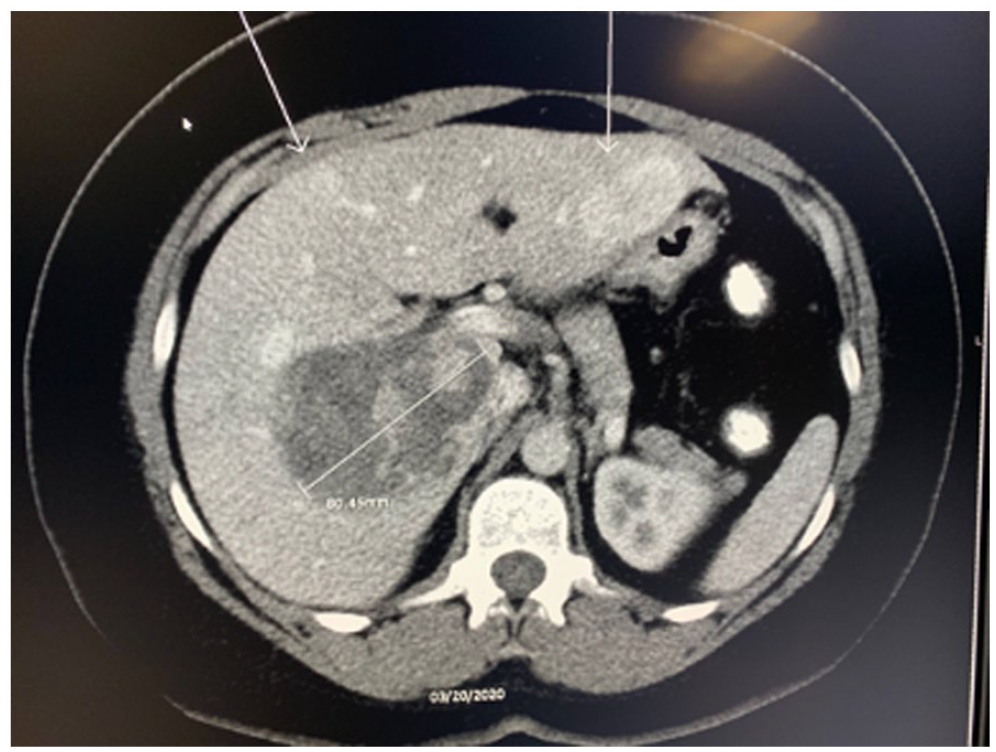
Computed tomography image revealing multiple lesions scattered throughout hepatic lobes.

Normal appearing hepatocytes without significant cytologic atypia, absence of bile ducts.

Preserved reticulin meshwork.
Discussion
The incidence of HA has been rising with the growing use of OCPs, increasing utilization of medical imaging, and rising incidence of obesity. 2 HAs are typically single lesions, but our patient presented with multiple lesions distributed in both lobes of the liver. HAs can present with RUQ abdominal pain but are discovered more commonly as incidental findings on routine imaging. 5 They are typically diagnosed by a liver biopsy with larger lesions having more pronounced pathological findings. The risk of post-liver biopsy hemorrhage is higher with large lesions, as was seen in our 2 patient. More caution is needed during and after liver biopsies in patients with large lesions and/or multiple lesions. The risk of malignant transformation of large HAs is greater than that of small lesions. 6 It is recommended that patients with multiple lesions be managed based on the size of the largest tumor due to the relationships between size, risk of bleeding, and malignant transformation. 7 Symptomatic lesions or lesions larger than 5 cm in size that are unresponsive to conservative management typically require surgical intervention.
HAs are managed with clinical observation, discontinuation of OCPs, and weight loss. Weight loss is highly recommended and strongly encouraged in patients with HAs. Some studies have shown that bariatric surgery is associated with HA regression and resolution. 8 The use of OCPs for 5 to 7 years carries a 5-fold risk of HA development while use of OCPs for 9 years or more leads to a 25-fold risk of HA development. 3 Discontinuation of OCPs usually leads to at least a 30% decrease in tumor size in 40% of patients. 9 Patients whose HAs are unresponsive to conservative management will require surgical resection.
Conclusion
In conclusion, our case illustrates that female patients with a history of obesity and long-term OCP use who present with multiple hepatic lesions need a high index of suspicion for HA. Clinically, post-liver biopsy vigilance in these patients is strongly advised to watch for complications including hepatic hemorrhage and hematomas.
Footnotes
Authors’ Note
This case report was presented at the ACG 2020 Annual Scientific Meeting as an online oral presentation in Nashville, Tennessee, via a digital e-Poster Hall on October 9, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.