
Abstract
Systemic sclerosis (SSc) is a disease that affects the gastrointestinal tract resulting in its atrophy and fibrosis of smooth muscles. Approximately 80% of SSc patients develop both gastroesophageal reflux disease (GERD) and dysphagia. The nocturnal GERD can cause regurgitation and aspiration, which can further aggravate the pulmonary fibrosis from SSc. Also, their dysphagia is further worsened by performing standard Nissen fundoplication. Therefore, we aimed to investigate whether Dor fundoplication (a 180° anterior wrap) can reduce nocturnal heartburn and regurgitation without worsening dysphagia in patients with SSc and severe GERD. Five SSc patients with drug-refractory severe GERD underwent a Dor fundoplication procedure with a median follow-up of 2 years (range: 1-5 years). In all 5 patients, the preoperative high-resolution manometry showed significant impairment of esophageal motility. Patients were interviewed postoperatively to assess for nocturnal and diurnal GERD symptoms, treatment response, the status of dysphagia, and adverse effects of surgery. The average age of 5 patients was 50 years and all were females. Four of the 5 patients (80%) reported 90% improvement in both diurnal and nocturnal GERD symptoms since surgery, with no nocturnal reflux, heartburn, or regurgitation, and reports to sleep at night without requiring any more pillows or wedges. About 50% of patients reported a decrease in their proton pump inhibitor dosage after surgery compared to before surgery. No surgical complication was reported and specifically, no worsening of dysphagia. The Dor fundoplication performed for refractory GERD in SSc patients substantially decreases heartburn and regurgitation, primarily nocturnal, without affecting dysphagia, thus improving the quality of life.
Keywords
Introduction
Systemic sclerosis (SSc) is the systemic form of scleroderma which is characterized by multisystem involvement with widespread vascular dysfunction and progressive fibrosis of the skin and internal organs. Gastrointestinal (GI) manifestations are the third most common presentation, after skin disease and Raynaud’s phenomenon. 1 Although any part of the GI tract can be affected, the esophagus is the most common organ being involved in up to 90% of the SSc patients.1-3 Scleroderma esophagus is defined as absent or ineffective peristalsis of the smooth muscle portion of the esophagus in combination with a hypotensive incompetent lower esophageal sphincter (LES).4,2 Due to the atonic smooth muscle dysfunction, the main manifestations of scleroderma esophagus are gastroesophageal reflux disease (GERD) and dysphagia.4,5 About 80% of the SSc patients develop GERD symptoms within 2 years of their diagnosis. 6 Severe GERD could result in other complications, such as peptic strictures (30%) and Barrett’s esophagus (37%).6-11 Furthermore, the nocturnal component of GERD may contribute to recurrent aspiration pneumonitis and subsequent pulmonary fibrosis. 12 Systemic sclerosis is also associated with gastric dysmotility and reduction in salivary production, resulting in impaired neutralization and clearance of refluxed gastric contents, particularly at night when the loss of effects of gravity worsens GERD.
Acid suppression with proton pump inhibitors (PPIs) is the standard of care to treat GERD in SSc patients, often requiring high doses. 13 Even though PPI may have a clinically significant short-term benefit, the long-term efficacy of these drugs is often not sustained. Schnoll-Sussman and Katz reported that the progression of esophageal dysfunction was not prevented with PPI use. 14 Furthermore, long-term acid suppression with PPI is associated with side effects such as small intestinal bacterial overgrowth, osteoporosis, and increased risk of cardiac events. 15
Surgical treatment is reserved for SSc patients with severe and refractory GERD. The most widely used surgical technique for GERD management in nonscleroderma patients is laparoscopic Nissen fundoplication. However, in the setting of SSc, studies showed an increased occurrence of postoperative dysphagia in up to 30% to 70% of patients. A Nissen fundoplication is also called a complete fundoplication by wrapping the gastric fundus entire 360° around the gastroesophageal (GE) junction. In contrast, a Dor fundoplication is a partial 180° wrap of the fundus around the GE junction and achieves good symptom resolution with no short-term complications. 16 There is still a lack of data on the Dor fundoplication in SSc patients. In this manuscript, we report our experience with the Dor fundoplication procedure on managing SSc-associated GERD.
Methods
We reviewed the preoperative and postoperative clinical course of SSc patients managed by one author (R.M.C.). These patients had refractory GERD, which is the presence of persistent heartburn, mostly nocturnal, even while being on high-dose PPIs and following lifestyle modification for GERD symptoms. Five of these SSc patients with drug-refractory severe GERD underwent the Dor fundoplication procedure, all performed by the same surgeon (B.D.). These patients were followed up long term with a median follow-up period of 2 years (range: 1-5 years). These study patients had a preoperative evaluation with a barium swallow, high-resolution manometry (HRM) study, and preoperative esophagogastroduodenoscopy (EGD). The variables that were measured postoperatively include nocturnal and diurnal GERD symptoms, functional status, quality of life, dysphagia symptom, and any adverse effects from surgery.
Surgical Technique
In 1962, surgeon Dor described a surgical technique in patients who underwent Heller myotomy for achalasia. To reduce the complications of reflux in these patients, an anterior 180° fundoplication was performed. 17 This procedure was modified using a robot-assisted approach to create a fundoplication that covers the right and the anterior portion of the esophagus, which anchors the gastric fundus to the diaphragmatic right hiatal rim. The initial steps in anterior Dor 180 are similar to laparoscopic and robotic approaches in Nissen. The sharp dissection of hiatus is achieved with a electro-cautery. The right crus is found upon dissection of the gastro-hepatic ligament, which is continued anteriorly up to the left gastric artery.
The dissection is continued across the hiatal apex, which would expose the left crus. The esophageal dissection is completed at the anterior mediastinum to ensure adequate intra-abdominal esophageal length. In case of absence of hiatal hernia, the posterior phreno-esophageal ligament is not dissected. Using interrupted braided nonabsorbable sutures, apparent herniation or diastasis of the anterior pillars of the crus are repaired. Then the anterior gastric fundus wall is sutured to the crural pillars and the diaphragmatic hiatus to create the anterior 180° Dor fundoplication.
The mobility of the gastric fundus (3-cm caudal and lateral to GE junction) is manipulated, so that it rests loosely in the front of the esophagus. The angle of His is recreated by placing seromuscular stitches through the right side of fundus and the left crural pillar. An apex suture is placed through the apex of the diaphragmatic hiatus apex and the top of the fundus. The posterior left fundus is then sutured to the right hiatal pillar to the level of the left gastric artery to complete the 180° fundoplication. As there is no risk of esophageal stenosis, the use of a rubber esophageal Bougie is not indicated.
Figure 1 depicts the laparoscopic operative picture during Dor fundoplication. The gastric fundus is sutured to the right hiatal pillar to the level of the left gastric artery to complete the 180° fundoplication. 18
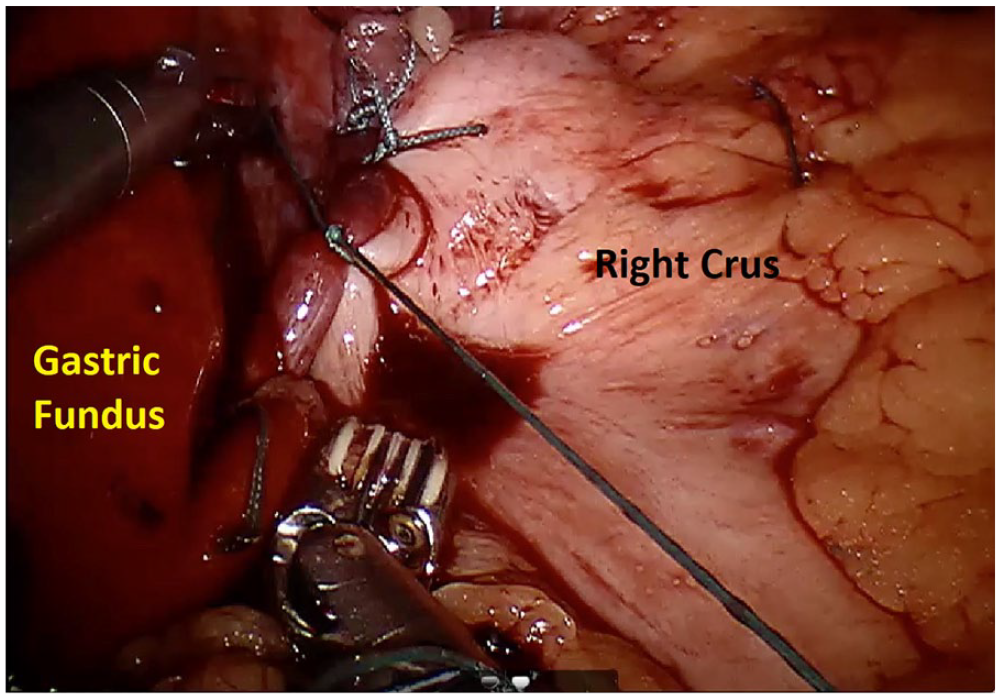
Depicts the laparoscopic operative Dor fundoplication demonstrating the gastric fundus sutured to the right hiatal pillar to the level of the left gastric artery to complete the 180° fundoplication.
Figure 2 shows a retroflexed view of the upper GI endoscopy, demonstrating an intact antireflux valve post-Dor fundoplication. 18 This retroflexed view through the upper GI endoscopy demonstrates the “partial wrap” of gastric muscle around the GE junction, which can be appreciated as a “snug” fit around the endoscope. This routine upper GI endoscopy is done to examine the partial fundoplication and to ensure that there is no esophageal or gastric injury during the surgery.

Shows the Dor fundoplication through a retroflexed view of the upper gastrointestinal endoscopy, confirming an intact antireflux valve post-Dor fundoplication.
A clear liquid diet as tolerated is started on a postoperative Day 1, and patients without oral intolerance or dysphagia on postoperative Day 2 are discharged with instructions to advance diet to full liquid and soft initially and then a regular diet during outpatient follow-up.
Ethical approval: all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
Study population and preoperative workup: Table 1 outlines the clinical profile and preoperative workup of the SSc patients undergoing Dor fundoplication surgery. All 5 patients were female with an average age of 50 years (range: 36-65). All patients had a barium swallow study which showed tertiary contractions with no peristalsis and a patulous GE junction. High-resolution manometry study in all the patients showed very impaired motility in the smooth muscle portion of the esophagus, essentially aperistalsis following wet swallows as well as an incompetent LES with pressures <10 mm of Hg (Figures 3 and 4). The preoperative EGD revealed a spectrum of findings ranging from esophagitis to Barrett’s metaplasia and hiatal hernia.
Demographics and Preoperative Diagnostic Testing Results.

Abbreviations: BMI, body mass index; GE, gastroesophageal; LES, lower esophageal sphincter.
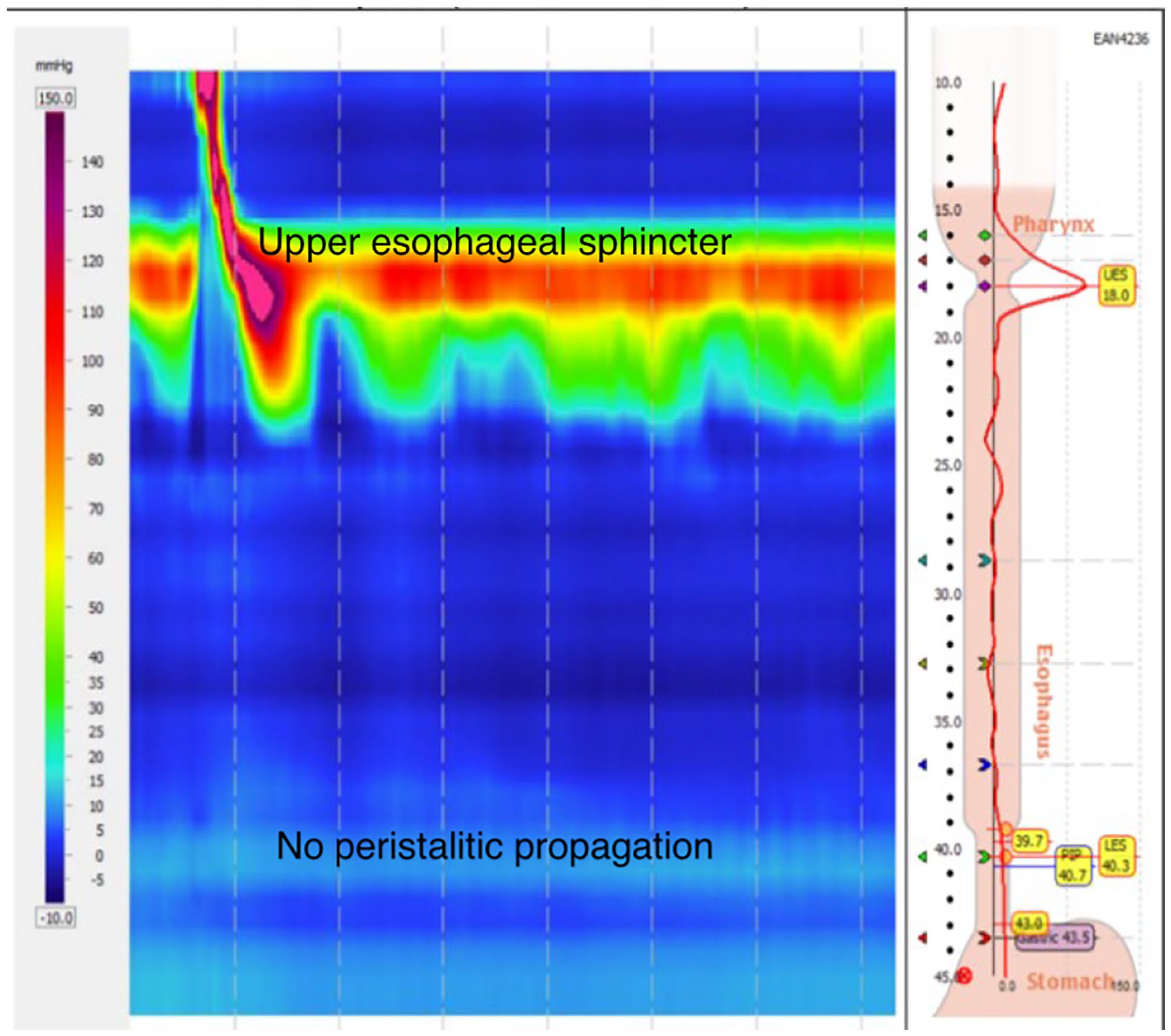
High-resolution esophageal manometry study results in scleroderma patients. In the scleroderma, in patients following wet swallow, there is normal upper esophageal sphincter relaxation and pharyngeal contraction, but there is no evidence of peristaltic propagation of the swallow through the smooth muscle portion of the esophagus in contrast to the normal study where there is propagation of the postswallow peristaltic wave into the distal esophagus ( See Figure 4).

High-resolution esophageal manometry study results in normal person with no abnormalities.
Surgery: The average Dor fundoplication procedure time was 140 to 150 min with an estimated blood loss of 15 to 20 mL. None of them had any immediate postoperative complications and were discharged by postoperative Day 2 after initially tolerating a clear liquid diet.
Postoperative outcomes: Table 2 outlines the postoperative improvement in GERD symptoms.
Assessment of Gastroesophageal Reflux (GERD) Symptoms Preoperatively and Postoperatively.

Dysphagia score symptoms: 1. Normal swallowing, 2. Difficulty on hard foods, but can swallow semisolids, 3. Unable to swallow any solids, but swallow liquids, 4. Difficulty swallowing liquids 5. Unable to swallow saliva.
Abbreviation: GERD, gastroesophageal reflux disease.
Postoperatively, 4 of the 5 patients reported a 90% improvement in both diurnal and nocturnal GERD symptoms since surgery. Also, they were able to sleep through the night without regurgitation or requiring any more pillows or wedges. Patients also reported a 50% decrease in their PPI dosage after surgery. On the global assessment, 4 of 5 patients identified a significant symptom improvement (of more than 90%), with the dominant change being a reduction in nocturnal regurgitation and improvement in sleep. There was no surgical complications, and none of the patient reported worsening dysphagia or symptoms of “gas bloat” syndrome. They were all able to belch and burp effectively after the surgery. These positive benefits were sustained during the long-term follow-up, up for 2 years. Furthermore, all these 4 patients reported that they would strongly recommend this surgery to another patient with GERD which is refractory to medical treatment. Only one patient did not perceive any sustained improvement in the GERD symptoms, however, there was no worsening dysphagia.
Discussion
Based on our experience, Dor fundoplication is effective in SSc patients with drug-refractory GERD symptoms. Our data emphasize that even in the setting of aperistalsis of the smooth muscle of the esophagus, this Dor fundoplication method does not worsen the dysphagia postoperatively.
The surgical treatment of GERD in SSc patients is challenging, and hence it is rarely performed. Previous studies have shown that in patients who underwent Nissen fundoplication, up to 70% of them experienced postoperative dysphagia due to worsening of their pre-existing esophageal dysfunction and essentially aperistalsis being induced by the relatively tight “wrap” at the GE junction.5,19,20 Hence partial fundoplication surgeries were preferred, in which the gastric fundus is wrapped to different degrees around the intraabdominal esophagus to recreate or augment the LES.5,21,22 The anterior fundoplication is the preferred procedure because it is simpler by obviating the need for extensive dissection in an inflamed or otherwise difficult operative field and thus avoiding the risk of left vagal nerve damage. The robotic approach provides better visualization and greater ease of use when compared to traditional laparoscopic surgery.
In conclusion, our data indicate that robotic Dor fundoplication performed for refractory GERD in SSc patients, substantially decreases heartburn and regurgitation, specifically nocturnal, thereby improving their sleep. The main limitations of our study were the small number of SSc patients in our series, but the positive aspects were a single surgeon (B.D.) performing all the procedures and one gastroenterologist (R.M.C.) evaluating and performing the preprocedural studies and clinical care, including the long-term follow-up.
We conclude that Dor fundoplication performed in SSc patients with refractory GERD, significantly decreases the heartburn and regurgitation, particularly the nocturnal symptoms, thereby providing a better quality of life. Furthermore, in our study, we did not have any complications and thereby provides an important treatment option in managing refractory GERD in scleroderma patients. Multicenter clinical trials will provide larger patient numbers in the future to validate the results of this study.
Footnotes
Acknowledgements
This study was accepted for a poster in the American college of gastroenterology (ACG) 2019 conference at San Antonio.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article