
Abstract
Hepatocellular carcinoma (HCC) is a primary liver malignancy known to occur majorly in patients with liver cirrhosis or those with a harbinger of risk factors like viral hepatitis, autoimmune liver disease, alpha-1 antitrypsin deficiency, alcoholic liver disease, and nonalcoholic fatty liver disease. The incidence of HCC has risen in the past 2 decades and currently ranks as the sixth most common cause of cancer-related death worldwide. Most cases are seen in adulthood, and only a very small percentage have been reported in adolescents with risk factors. The 2 pathologic subtypes of pediatric HCC are classic and fibrolamellar. Here, we discussed a very interesting rare case of a healthy male teenager with no apparent liver disease or risk factor who presented with right-upper-quadrant pain, normal alpha-fetoprotein level, and abdominal ultrasound showing a large hepatic mass. A liver biopsy was positive for HCC with fluorescent in situ hybridization showing a PRKACA complex gene pattern, favoring the fibrolamellar type.
Introduction
Primary liver tumors are rarely seen in childhood and constitute about 1% of all solid tumors in that age group. 1 The second most common liver tumor after hepatoblastoma in childhood is hepatocellular carcinoma (HCC). Only about 0.5% to 1% of patients younger than 20 years have been identified with this malignancy. 2 The median age of diagnosis is 58 years. Fibrolamellar type comprises about 1% to 9% of all HCCs according to Surveillance, Epidemiology, and End Results database and is often seen in patients aged between 10 and 35 years with no primary liver disease. 3 It was first described in 1956 by Edmondson in a 14-year-old female with no background liver disease. 4 In children and teenagers, hepatitis B infection acquired perinatally, human immunodeficiency virus (HIV), and inherited metabolic disorders have been identified as risk factors for HCC but rarely contribute to fibrolamellar type. Hence, <10% of patients have cirrhotic liver morphology. 3 Due to the low frequency of fibrolamellar type, no randomized controlled trial has been done to explain the most successful regimen for treatment. In most cases, children present with an advanced tumor that may not be amenable to surgical resection. Hence, liver transplants and nonsurgical modalities are considered in late-presenting patients.
Case Presentation
A male teenager with no significant past medical history presented to the emergency department with 2 weeks of diffuse abdominal pain and intermittent nonbilious vomiting, associated with unintentional weight loss of about 20 lbs over the preceding 3 months. He denied a family history of cancer. Examination findings were significant for a body mass index of 36 kg/m2 (18.5-24.5) and epigastric tenderness. Hepatitis viral screening, HIV, CA 19-9, ceruloplasmin, and lipase were unremarkable. Other laboratory investigations are shown in Table 1. Abdominal ultrasound (US) showed diffuse heterogenicity of the liver with a large mass in the left hepatic lobe and sludge in the gall bladder with no shadowing stones. Further imaging was pursued with contrast-enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) of the abdomen that confirmed a large heterogeneous mass in the lateral-segment left lobe of the liver measuring 12 × 6.5 cm, an extensive portal vein thrombosis, portal, and peripancreatic lymphadenopathy which were concerning for malignant cause (Figures 1 and 2). With a high suspicion of a malignant lesion versus lymphoma in mind, we obtained a CECT of the chest which showed enlarged paracardial and paraesophageal lymph nodes but no lung nodules. Computed tomography (CT) neck and soft tissue revealed multiple nonenlarged cervical lymph nodes. A biopsy of the hepatic lesion guided by CT was then obtained, which revealed lobular aggregates of hepatocytes with moderate nuclear atypia and disorganization and strong stain expression for the hepatocyte stain (hep par 1) and cytokeratin 7, while glypican 3, CD 10, and Carcinoembryonic antigen (CEA) were negative, confirmatory for HCC (Figures 3-5). The patient was referred to oncology for chemotherapy because the size of the liver mass and portal vein involvement excluded him from benefiting from resection or transplant. During the follow-up visit 2 months later, genetic testing with fluorescent in situ hybridization (FISH) studies demonstrated a positive PRKACA complex pattern gene rearrangement which was in favor of the fibrolamellar subtype.
Patient’s Laboratory Test Results.

Abbreviation: ESR, Erythrocyte sedimentation rate; INR, International normalized ratio; HCG, Human chorionic gonadotropin.
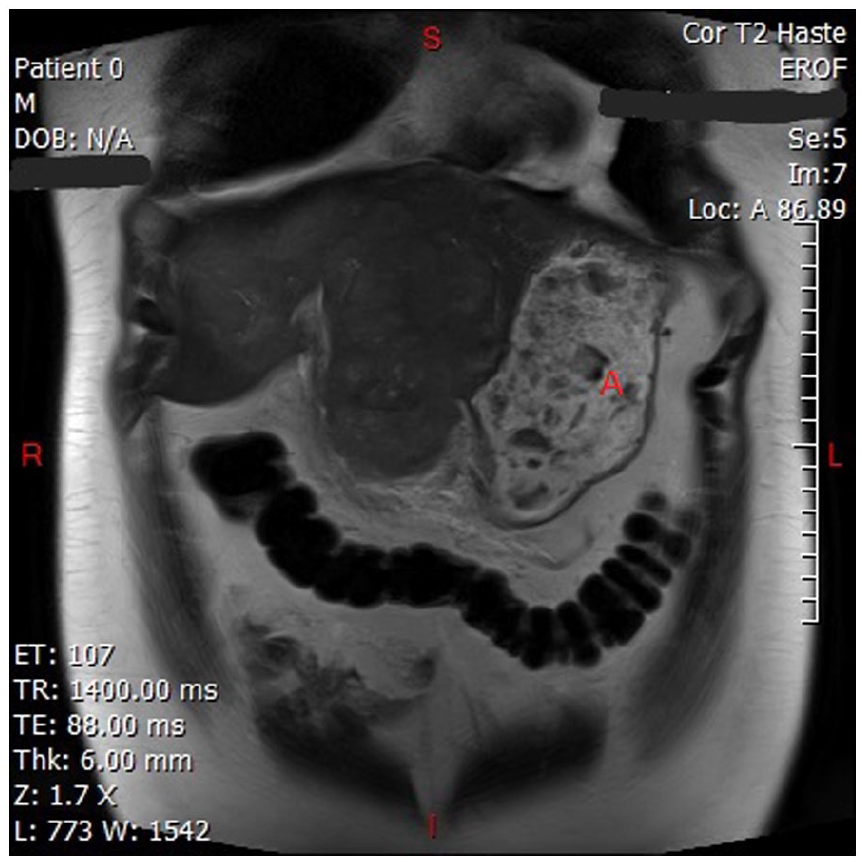
Multiphasic MRI showing hepatic mass (letter A).

Multiphasic MRI showing portal vein thrombosis (letter c) and heterogenous hepatic mass (blue arrow).

(A) (B) Cytology smear with Diff-Quik stain showing nests of malignant cells with increased nuclear-cytoplasmic ratio and marked nuclear pleomorphism.

(A) Routine hematoxylin and eosin staining of FFPE biopsies at increasing magnification displaying malignant cells diffusely distributed throughout the sample. (B) High-power view of malignant cells infiltrating the stroma with strong nuclear staining and mitotic figures within pleomorphic nuclei.

Immunohistochemical staining of tissue biopsy: (A) Broad positivity (brown) for hepatocyte stain of the malignant cells. (B) Strong focal positivity (brown) of the malignant cells for cytokeratin-7. (C) Negative staining for glypican throughout the tissue sample.
Discussion
The pathophysiology of HCC in adults and children is not well understood. There are 2 distinct mechanisms of HCC in adolescents. First is in the setting of liver cirrhosis, viral hepatitis, HIV infection, alpha-1 antitrypsin deficiency, biliary atresia, progressive familial intrahepatic cholestasis, metabolic disorders like tyrosinemia, and glycogen storage diseases. Second is the sporadic HCC that occurs in the absence of any liver disease or infections as seen in our patient. Hepatocellular carcinoma in adolescents is commonly associated with huge hepatomas, portal vein thrombosis, and distant metastasis at the time of diagnosis. Due to the rarity of this malignancy in childhood, it can easily be misdiagnosed with conditions like hepatoblastoma, focal nodular hyperplasia, abscess, hepatic adenoma, primary hepatic lymphoma, and undifferentiated embryonal sarcoma. Pathologically, the 2 most common types of HCC seen in children are classic and fibrolamellar. In comparison to classic HCC, patients with fibrolamellar have no cirrhosis or hepatitis, are younger, caucasian, and less likely to have positive Alpha-fetoprotein (AFP). 5 The above description fits with our case, hence favoring the fibrolamellar type. A novel DNAJB1-PRKACA genetic fusion due to 400-kb deletion was recently discovered in the fibrolamellar variant of HCC. 6 The fusion of these genes results in the upregulation of a chimeric protein that plays a role in the tumorigenesis of fibrolamellar carcinoma (FLC). Hence, about >95% of FLCs have been documented to have this genetic fusion. 7 The study by Vyas et al detected about 5 pancreatic neoplasms with DNAJB1-PRKACA fusion similar to the structural variant observed by Honeyman et al 6 in their seminal study, thus raising awareness that this genetic fusion is not unique to FLC and may also be seen in pancreaticobiliary neoplasms. 8 In our case, PRKACA FISH was manually performed with the analysis of 60 cells using the PRKACA spectrum orange (centromeric) and the PRKACA spectrum green (telomeric) probes, and the result showed a complex pattern with a significant number of cells demonstrating unpaired green signals. While not entirely specific, a similar pattern was reported by Vyas et al 8 ; thus, next-generation sequencing studies may be considered to confirm the presence of this translocation. The first screening modality for HCC is US. No recommendation currently exists for screening of patients with no liver cirrhosis for HCC; however, due to the increased prevalence of Hepatitis B virus (HBV)-induced HCC in the young population, American Association for the Study of Liver Diseases (AASLD) recommends surveillance in black, Asian men, and women with HBV infection from ages 20, 40, and 50 years, respectively. 9 Multiphasic CT and MRI are gold-standard imaging modalities for diagnosing HCC. The stage of diagnosis of HCC is the most important factor determining patients’ survival. Patients with small, localized tumors can be treated with resection, ablation, or liver transplant with excellent long-term survival. Those with large, macrovascular invasive tumors with extrahepatic metastasis benefit from palliative chemotherapy. Several criteria have been used to risk stratify patients that would benefit from a liver transplant: the Milan criteria (1 tumor ≤5 cm, maximum of 3 total tumors with none >3 cm) and the University of California, San Francisco, (UCSF) criteria (single tumor <6.5 cm, maximum of 3 total tumors with none >4.5 cm, and cumulative tumor size <8 cm). Attempts have been made by studies to expand the Milan criteria using UCSF to accommodate more patients for a liver transplant; however, it was challenged due to the small sample size. 10 Our patient did not meet any of the above criteria considering the liver mass size of 12 × 6.5 cm, thus chemotherapy with atezolizumab plus bevacizumab was recommended. The IMBrave 150 study by Cheng et al demonstrated statistically significant and clinical improvement in both overall and progression-free survival for atezolizumab + bevacizumab versus sorafenib in patients with unresectable HCC who have not received prior systemic therapy. 11 Although patients with FLC were not included in the above study, De Toni and Roessler reported a case of a 22-year-old female with metastasized FLC who demonstrated a near-complete response of all tumor lesions after 4 cycles of treatment with dual immune checkpoint inhibitors. 12 Hepatocellular carcinoma in adolescents tends to be more advanced than that in adults; thus, prompt risk stratification with the initiation of adequate treatment is recommended once diagnosed.
Footnotes
Author contributions
A.E. evaluated this patient and presented the case to O.U. and Y.P. who did literature review and wrote the manuscript and then submitted it to A.A. and P.P. for final review and corrections. V.M. read the pathology slides while L.L. provided pathology slides with explanatory captions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient’s parents for their anonymized information to be published in this article.
Article Guarantor
Onyinye Ugonabo