
Abstract
Isolated pancreatic metastases from melanoma are rare with high mortality rate and account for less than 1% of metastatic melanomas. Treatment options are limited with highest overall survival reported in those with complete surgical resection. Of cases reported in the literature with nonsurgical management, highest length of survival was reported to be 10 months. We report a case of malignant melanoma with isolated pancreatic metastasis treated with interferon therapy and immunotherapy, with evidence of progressive tumor shrinkage and survival at 38 months.
Introduction
Pancreatic adenocarcinoma is the most common tumor of the pancreas. Pancreatic metastases are rare and account for 2% to 5% of pancreatic malignancies.1,2 The most common primary malignancies that metastasize to the pancreas are renal, lung, breast, and colon cancer. Isolated pancreatic metastases from melanoma are rare with high mortality rate and account for less than 1% of metastatic melanomas, making it a diagnostic challenge. 3 Given difficulty of differentiating primary tumors from metastases based on imaging findings, it is crucial to obtain endoscopic ultrasound (EUS) with fine needle aspiration (FNA) for accurate diagnosis. 1 Treatment options are limited with generally poor response rates to conventional chemotherapy. Prior studies have shown improved 5-year survival rates in those with complete surgical resection of isolated pancreatic melanoma metastases compared to those with incomplete resection and nonsurgical treatment. 4 There are several reports of pancreatic metastasis from malignant melanoma reported in the English medical literature; of those treated nonsurgically, longest length of survival was reported to be 10 months. 5 Here, we present a unique case of malignant melanoma with isolated pancreatic metastasis diagnosed by EUS-FNA, treated nonsurgically with immunotherapy, with evidence of tumor shrinkage and survival at 38 months.
Case Presentation
A 75-year-old male with a past medical history of prostate cancer status post (s/p) radiation therapy and cutaneous melanoma s/p resection 24 years prior presented to the emergency department with progressively worsening jaundice, unintentional weight loss, dark urine, pale stools, and nausea. On initial presentation, vital signs were as follows: body temperature 37.1°C, blood pressure 128/82 mm Hg, heart rate 87 beats/min, respiratory rate 16 breaths/min, and oxygen saturation 98% on room air. Physical examination was notable for scleral icterus, generalized jaundice, and no skin lesions concerning for recurrent melanoma. Initial laboratory work up including complete blood count (CBC) and comprehensive metabolic panel (CMP) were notable for total bilirubin 14.0 mg/dL, direct bilirubin 11.5 mg/dL, aspartate aminotransferase (AST) 1549 u/L, alanine aminotransferase (ALT) 1682 u/L, alkaline phosphatase (ALP) 3898 u/L, and lipase 1300 u/L. Computed tomography (CT) of the abdomen and pelvis demonstrated a 4.4 × 4.0 × 3.7 cm pancreatic head mass with biliary obstruction and dilated biliary ducts (Figure 1A). Patient subsequently underwent EUS with biopsy of pancreatic head mass. Endoscopic ultrasound showed a 38 × 36 mm hypoechoic lesion in the pancreatic head with invasion of the portal vein and portal vein thrombosis. Immunohistochemical stains for S-100 protein, Human Melanoma Black (HMB45), melanoma antigen recognized by T-cells 1 (MelanA), and SRY-related HMG-box 10 (SOX10) were performed. The tumor cells were positive for S-100, HMB45, and SOX10. Histopathology and immunohistochemical studies were diagnostic for melanoma and indicative of metastatic disease to the pancreas. Genetic testing was further positive for a BRCA1 gene mutation. General surgery was consulted, and patient was deemed a poor surgical candidate due to tumor invasion of the portal vein. Subsequently, an internal/external biliary drainage catheter was placed, and patient was discharged with outpatient follow-up with oncology. Positron emission tomography (PET)-CT did not show other sites of disease activity. Patient received 1 month of interferon (IFN) therapy followed by immunotherapy consisting of nivolumab and ipilimumab. He was unable to tolerate dual immunotherapy and was thereafter switched to monotherapy with nivolumab. After 12 months of treatment, repeat CT of the abdomen and pelvis demonstrated a decrease in the pancreatic head mass to 3.6 × 2.0 cm (Figure 1B). Repeat CT of the abdomen and pelvis at 24 months showed progressive decline in size of pancreatic head mass to 1.6 × 1.6 cm (Figure 1C). Latest CT at 38 months postdiagnosis and initiation of treatment demonstrated pancreatic head mass measuring 1.6 × 1.0 cm with no ductal dilatation (Figure 1D). Biliary drain was removed; liver function tests improved, and patient continues to receive immunotherapy every 2 weeks.
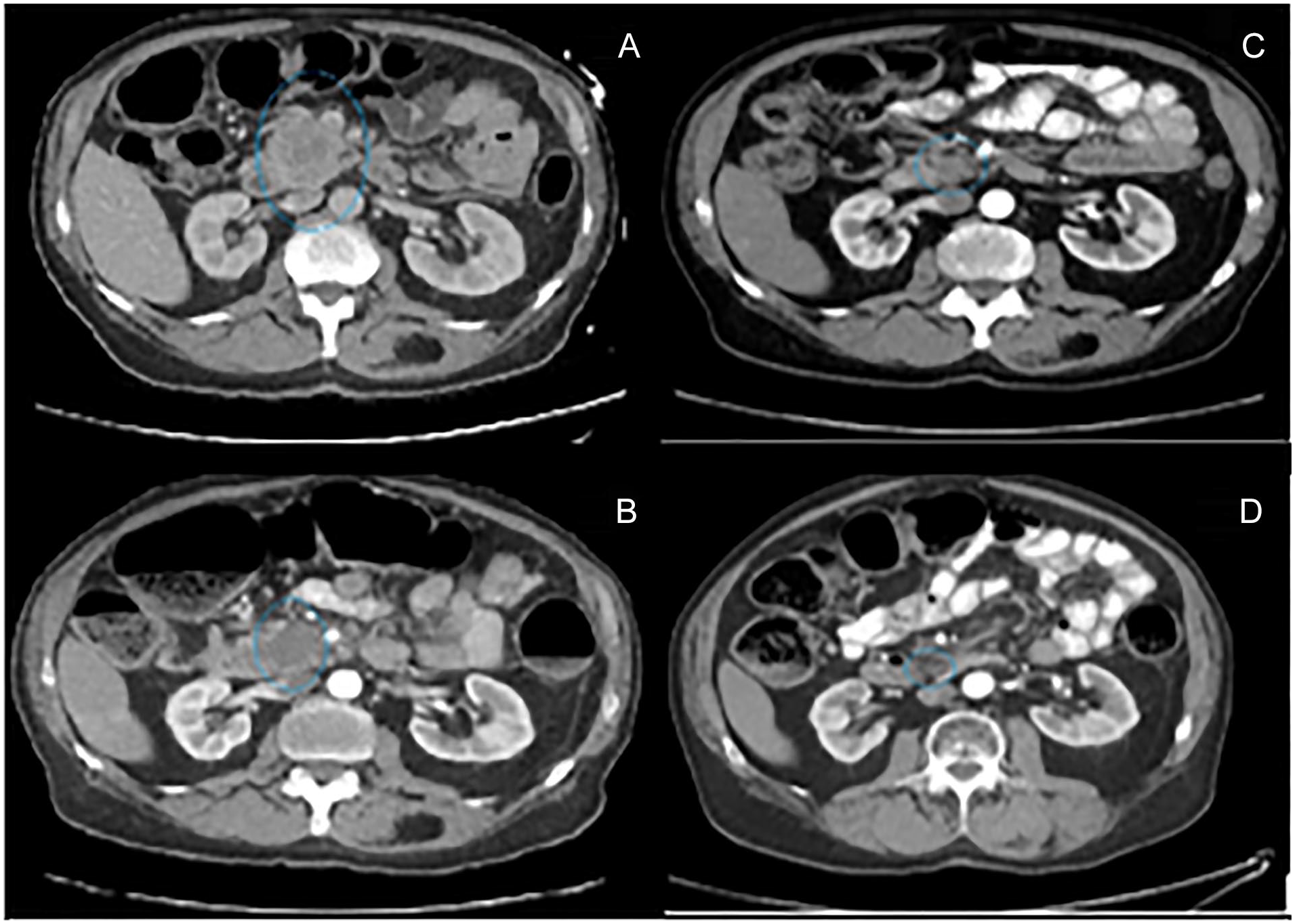
Serial computed tomography of the abdomen and pelvis. (A) 4.4 × 4.0 cm pancreatic head mass at time of diagnosis. (B) 3.6 × 2.0 cm pancreatic head mass at 12 months. (C) 1.6 × 1.6 cm pancreatic head mass at 24 months. (D) 1.6 × 1.0 cm pancreatic head mass at 38 months.
Discussion
Metastatic melanoma has a poor prognosis with a 5-year survival rate of less than 5%. Although melanomas frequently metastasize to the gastrointestinal system, metastasis to the pancreas renders an even worse prognosis. Life expectancy in malignant melanoma with gastrointestinal metastases is typically 6 to 12 months. 6 The debate for surgical approach versus chemotherapy management of patients with malignant melanoma with isolated pancreatic metastasis is controversial due to lack of data and very rare occurrence. In our patient’s case, given invasion of the portal vein, a complete surgical resection was not feasible. In one study, 60 patients with malignant melanoma with metastatic disease to intra-abdominal solid organs underwent surgical resection; it was demonstrated that the 5-year survival rates for patients with surgical resection was 37.5% (median survival time of 23.8 months) as opposed to nonsurgical approach with 5-year survival rate of 23% (median survival time of 15.2 months). 7 Upon review of the literature, we found 83 cases of pancreatic metastases from malignant melanoma reported in the English medical literature. Of these 83 cases, 72 patients underwent surgical resection with longest length of survival reported to be 228 months. 2 Management was not reported in 3 cases. The remaining 8 cases were treated with a nonsurgical approach with highest length of survival reported to be 10 months (Table 1).
Metastatic Malignant Melanoma of Pancreas Reported in the English Literature.

Abbreviations: NR, not reported; EUS-FNA, endoscopic ultrasound fine need aspiration; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography.
Our patient is alive at 38 months following treatment with combination IFN therapy and immunotherapy with evidence of progressive tumor shrinkage. Interferon is typically utilized as an adjuvant therapy in patients with malignant melanoma who underwent surgical resection. 14 The use of IFN in metastatic melanoma is controversial; however, IFN combined with novel biological and immunotherapies has been shown to have a synergistic effect with improved patient outcomes. 14 Furthermore, the discovery of immune checkpoint inhibitors such as ipilimumab and nivolumab have further contributed to better patient outcomes with studies showing significantly improved progression-free survival in those with previously untreated metastatic melanoma. In a study by Larkin et al, 15 patients with unresectable stage III and IV malignant melanoma were demonstrated to have median progression-free survival of 11.5 months on combination nivolumab and ipilimumab therapy. In a study by Postow et al, 16 patients with metastatic melanoma treated with nivolumab and ipilimumab were demonstrated to have a 61% overall response rate compared to patients treated with placebo. Although the utility of checkpoint inhibitors such as nivolumab and ipilimumab in the treatment of metastatic melanoma is a relatively late discovery, recent studies have shown significantly higher success rates and ultimately changed the velocity of the disease.
To our knowledge, our case is the first to report survival at 38 months in a patient with isolated pancreatic metastasis from malignant melanoma treated nonsurgically with combination IFN and immunotherapy. This case demonstrates the importance of including metastatic melanoma in the differential diagnosis of all patients presenting with pancreatic masses as prompt treatment with immunotherapy can render better outcomes even in those who are not surgical candidates.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Ethics Approval
Our institution does not require ethical approval for reporting individual case or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.