
Abstract
Primary ovarian non-Hodgkin lymphoma is a rare lymphoma that is often associated with diagnostic delays, initial misdiagnosis, and inappropriate management. We report a case of ovarian diffuse large B-cell lymphoma (DLBCL) in a young female who initially presented with generalized fatigue, lower abdominal discomfort, and 40 pounds of unintentional weight loss. She subsequently had a computed tomography of abdomen done that showed fatty liver, hepatomegaly, and a left heterogeneous ovarian mass measuring about 4 × 4.2 cm. Transvaginal ultrasound was also done that showed a heterogeneous solid left adnexal mass measuring 7.4 × 5.6 × 6.6 cm. She subsequently had a total abdominal hysterectomy with bilateral salpingo-oophorectomy. Immunohistochemistry (IHC) showed the malignant cells expressing PAX5, CD20, and BCL2 with a Ki-67 proliferation index greater than 90%. The cells were negative for AE1/AE3, S100, CD30, and cyclin D1. Aggressive B-cell lymphoma fluorescence in situ hybridisation (FISH) panel was positive for rearrangement of BCL6 and MYC, with no evidence of BCL2 rearrangement, consistent with a double-hit high-grade B-cell lymphoma. Immunohistochemistry for BCL6 and MU M1 showed positive staining in the malignant cells. CD10 was negative. The staining profile was consistent with nongerminal center B-cell-like type of DLBCL. Ovarian lymphoma is a very rare entity; the presence of an enlarged ovarian tumor should raise the suspicion of ovarian lymphoma, and our case also emphasizes on the use of IHC markers in diagnosing the ovarian DLBCL.
Introduction
Primary ovarian non-Hodgkin lymphoma is a very rare and uncommon entity. It accounts for about 1.5% of all ovarian tumors and 0.5% of all the non-Hodgkin lymphomas (NHLs). The most common histologic subtype of primary ovarian NHL is diffuse large B-cell lymphoma (DLBCL) that accounts for approximately about 20% of all primary ovarian lymphomas. DLBCL is an aggressive and heterogeneous 1 group of NHL that typically present with a rapidly enlarging symptomatic mass, most usually nodal enlargement in the neck or abdomen, but may present as a mass lesion anywhere in the body. The most common primary extranodal disease sites involving the DLBCL are the gastrointestinal tract, thyroid, kidneys, breast, liver, testis, adrenals, uterine cervix, and tonsil but rarely involve the ovaries. 2 Ovarian DLBCL is a rare, complex type of lymphoma that harbors a favorable prognosis per studies. The 5-year survival is approximately 70% in ovarian lymphoma per one of the case study series. 3
Case Presentation
A 48-year-old female presented to her primary care physician with generalized fatigue, lower abdominal discomfort, and 40 pounds of unintentional weight loss. Computed tomography of the abdomen done showed fatty liver, hepatomegaly, and a left heterogeneous ovarian mass measuring 4 × 4.2 cm (Figure 1) and an enlarged left adrenal gland measuring 1.5 × 2 cm. Transvaginal ultrasound done showed a heterogeneous solid left adnexal mass measuring 7.4 × 5.6 × 6.6 cm. She subsequently had a total abdominal hysterectomy with bilateral salpingo-oophorectomy. Her pathology showed that the left ovary displayed near-complete replacement by a diffuse proliferation of large somewhat pleomorphic cells (Figure 2), with prominent nucleoli (Figure 3), numerous mitotic figures, admixed body macrophages, and punctate areas of necrosis. Immunohistochemistry showed the malignant cells expressed PAX5, CD20, MYC (Figure 4), and BCL2 (weak 30%). Her Ki-67 proliferation index was greater than 90% (Figure 5). The cells were negative for AE1/AE3, S100, CD30, and cyclin D1. An aggressive B-cell lymphoma FISH panel was positive for rearrangement of BCL6 and MYC, with no evidence of BCL2 rearrangement; the findings are consistent with the diagnosis of high-grade B-cell lymphoma/double-hit lymphoma with MYC and BCL2 and/or BCL6 rearrangements by the World Health Organization classification. Immunohistochemistry for BCL6 and MU M1 showed positive staining in the malignant cells. CD10 was negative. The staining profile was consistent with nongerminal center B-cell-like type (non-GCB/ABC) of DLBCL. Final pathology results confirmed high-grade CD20-positive DLBCL of the left ovary. A positron electron tomography (PET) scan showed abnormal uptake within a soft-tissue density structure in the right maxillary sinus. She was categorized as stage IV Lugano modification of the Ann Arbor Stage due to the involvement of the right maxillary sinus. She received dose-adjusted DA-EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, rituximab). Positron electron tomography scan after 3 cycles showed interval resolution of hypermetabolic polypoid lesions of the right maxillary sinus. She completed total 6 cycles of DA-EPOCH-R. She is currently being monitored with serial PET scans and continues to be in remission after 1.5 years without any evidence of relapse.

Left adnexal mass measuring about 4 × 4.2 cm on computed tomography of the abdomen and pelvis.
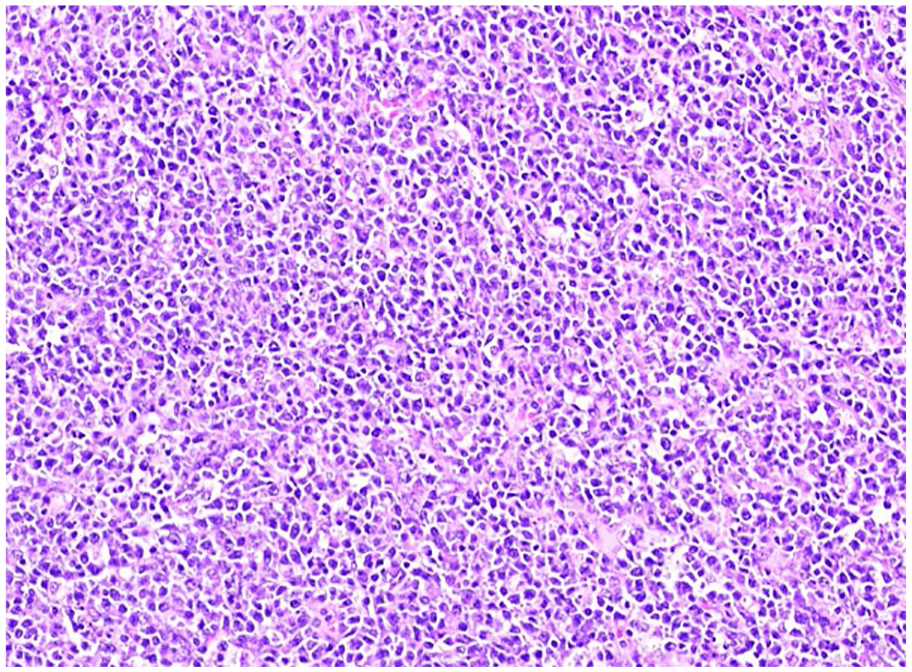
Hematoxylin & eosin–stained section of the ovarian mass showing a diffuse proliferation of large somewhat pleomorphic cells. Photographed at 20× magnification.
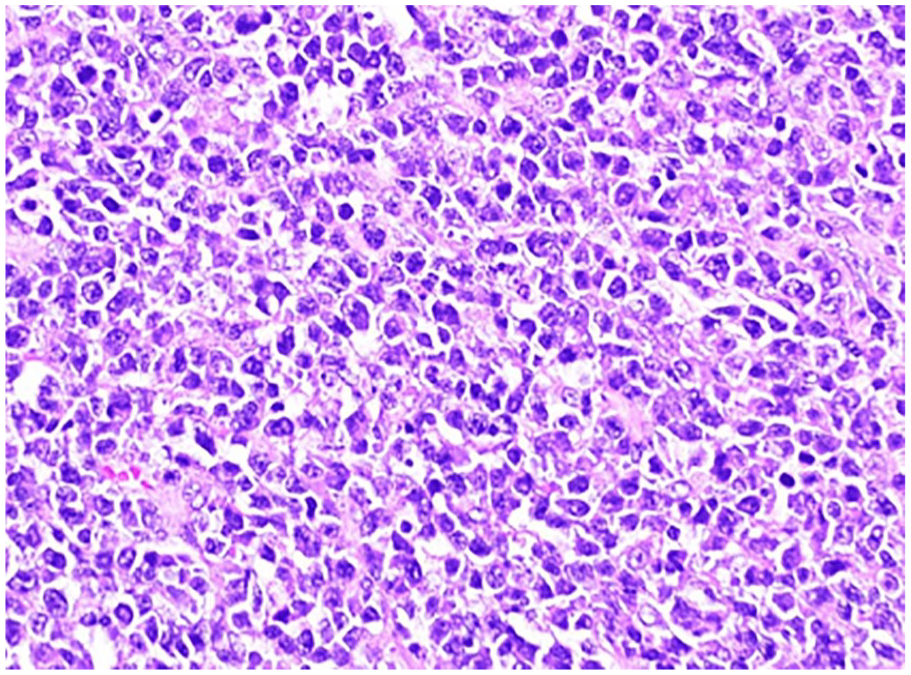
Hematoxylin & eosin–stained section of the ovarian mass photographed at 40× magnification showing the irregular nuclear contours and prominent nucleoli.

Ovarian mass photographed at 20× magnification stained with Ki-67 immunohistochemistry showing the high proliferation index with >90% of the cells staining positive (brown = positive).

Ovarian mass photographed at 20× magnification stained with MYC immunohistochemistry showing expression in about 50% of the cells (brown = positive).
Discussion
We report a rare case of primary ovarian non-GCB/ABC DLBCL. Ovarian DLBCL only accounts for about 0.5% of total cases of NHL. 4
Primary ovarian lymphoma are most often reported in young women with a median age of 33 to 42 years.5,6 Bilateral involvement has been previously reported in approximately 38% to 71% of cases.3,6 The clinical presentation of ovarian lymphoma can vary among abdominal mass, irregular vaginal bleeding, abdominal pain, fever, fatigue, or night sweat’s (B symptoms) or sometimes ascites or pleural effusion. Palpable liver and splenomegaly can also be found on physical examination.
Extranodal sites with C-MYC and BCL2/BCL6 translocations include the liver, central nervous system (CNS), ribs, breast, intestine, sacrum, and stomach and rarely the ovaries. 7 Ovarian lymphomas are extremely rare due to the lack of lymphoid tissue in the ovary. The ovarian lymphoma may have its origination from the chronic inflammatory cells as a result of the pelvic inflammatory disease in the ovary or from the lymphoid aggregates in the corpus luteum or from the vessels of ovarian hilum. 8 There are different perspectives regarding the origin of a primary ovarian lymphoma, which include its origin from the lymphoid tissues that already exist in the ovary, 9 or that there are tumor-derived cells around the hilum of the ovary or the corpus luteum cells in the form of blood vessels, 10 or the pelvic inflammatory disease and endometriosis or autoimmune diseases, causing chronic ovarian inflammation from the reactive lymphocytes and aggregation lymphocytes, which in turn results in the malignant transformation. 11
DLBCL is the most common type of lymphoma in the ovary, accounting for about 20% of the total ovarian lymphomas, followed by Burkitt lymphoma. 12 An overall 5-year survival of 70.0% has been documented in primary ovarian DLBCL based on few case studies,3,12 whereas when detected late, due to a delayed or inaccurate diagnosis, the primary ovarian DLBCL has a poorer outcome with a range of 0 to 36% of patients expected to survive for less than 3 years.
Studies have demonstrated superior outcomes with dose-adjusted EPOCH-R compared with standard chemotherapy like R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).13-15 Our patient was treated with 6 cycles of dose-adjusted EPOCH-R, with subsequent PET scan showing complete remission. Because patients with MYC-rearranged lymphoma have an increased risk of CNS involvement, she was also treated with intrathecal methotrexate for CNS prophylaxis. Following her up for the last 1.5 years, the patient is still in good condition without any relapse.
In conclusion, ovarian lymphoma is very uncommon, and it is very difficult to diagnose the primary ovarian lymphoma not only due to its rarity and its similarities with other female genital system malignancies but also due to nonspecific clinical manifestations. The failure to establish an accurate early clinical, histopathological diagnosis leads to inappropriate management of these patients and unnecessary treatment delays. The presence of an enlarged heterogeneous ovarian mass should always raise the suspicion for ovarian lymphoma, and immunohistochemistry should be utilized for differentiation from other ovarian tumor histopathologies for an appropriate diagnosis. To our knowledge, this is a rare presentation of DLBCL/high-grade B-cell lymphoma with MYC and BCL6 translocation involving the ovaries. There is a need for the physicians and especially oncologists to be aware of aggressive primary ovarian lymphomas so that early diagnosis can be made and correct multiagent chemotherapy can be initiated in a timely manner.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Prior Presentation of Abstract Statement
Urella, Madhulika; Nwanwene, Kemnasom; Sidda, Adarsh; and Pacioles, Toni: A Rare Case of Primary Ovarian Diffuse Large B-cell lymphoma. Poster presented at Marshall Research Day, Huntington, West Virginia, October 2021.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was obtained from the patient.