
Abstract
Colorectal cancer (CRC) is the third most common malignancy and the second most common deadly cancer worldwide as of 2020. Unusual presentation of this cancer with locally advanced disease is rare and seen in only 5% to 22% of cases. We present the case of a 53-year-old male who had invasive cecal adenocarcinoma with phlegmon of the abdominal wall musculature at presentation and an aggressive course that did not respond to the standard lines of therapy. In the current era of ongoing tremendous developments in colorectal cancer diagnosis and treatment, this uncommon case reminds us that locally advanced CRC is still a challenge to manage. Precision medicine with treatment strategies tailored to an individual’s genetic, environmental and lifestyle factors is the current need.
Keywords
Case Description
A 53-year-old male presented with a gradually worsening right lower quadrant abdominal mass with discomfort, weight loss, and occasional blood in stool. History is significant for a 10-pack-year smoking history and colorectal cancer in mother and maternal grandfather after 60 years of age. Physical examination revealed pallor and a 15 × 15 cm firm, non-tender, non-mobile right lower quadrant abdominal mass with intact bowel sounds. Initial labs were remarkable for anemia due to chronic disease and iron deficiency and elevated carcinoembryonic antigen (CEA). Colonoscopy revealed a frond-like, friable, fungating non-circumferential and non-obstructing large mass in the cecum. Biopsy of the mass was moderately differentiated invasive adenocarcinoma. Contrast-enhanced CT abdomen and pelvis showed wall thickening of the cecum and proximal ascending colon with pericecal inflammation extending into right iliopsoas and abdominal wall musculature with no discrete abscess (Figure 2). Tumor board discussion suspected the phlegmon to be of malignant origin, but the initial biopsy showed only inflammatory pathology. As per eighth edition AJCC (American Joint Committee on Cancer) TNM classification, initial stage was I, T2N0M0. As the tumor was inoperable, patient was started on neo-adjuvant chemotherapy with FOLFOX to make it resectable. After cycle 1, patient got admitted with distal small bowel obstruction with transition point at the mass and underwent emergent right hemicolectomy with 30 cm ileal resection and primary anastomosis (Figure 1). Surgical pathology showed T3 moderately differentiated colon cancer, 34 lymph nodes evaluated with none being positive, uninvolved margins, positive focal lymphovascular invasion, no perineural invasion, and no tumor deposits. Tumor reclassified to high risk stage IIa, T3N0M0 due to obstruction. Immunohistochemistry detected heterozygous mutation in K-ras codon 12 while NRAS and MSI were negative. Patient was continued on FOLFOX regimen. Repeat imaging after 6 cycles of FOLFOX showed progression of soft tissue invasion suggesting localized spread of disease corroborating with rise in CEA levels. Owing to progression of disease, patient underwent cytoreductive surgery and hyperthermic intraperitoneal chemotherapy with 30 mg of mitomycin C. Based on operative pathology, tumor was restaged to IVC, any T, any N, M1c and chemotherapy with FOLFIRI was initiated. After 2 cycles, CT scan showed further local progression with abscess formation in the right lower quadrant (requiring admission to hospital) and enlarged right pelvic and inguinal lymph nodes concerning for metastatic lymphadenopathy. CT chest showed pulmonary nodules, presumably metastatic. Tumor was considered incurable, and given that tumor is primarily locally recurrent, patient was started on palliative radiotherapy to the tumor mass with capecitabine. Subsequent to radiotherapy, patient was started on third line trifluridine/tipiracil and bevacizumab. However, an enterocutaneous fistula developed at the tumor site eventually and patient opted for hospice care (Figure 3).

Hemicolectomy specimen.

Axial slice of CT Abdomen and Pelvis with oral and IV contrast showing soft tissue inflammation in the right lower quadrant.
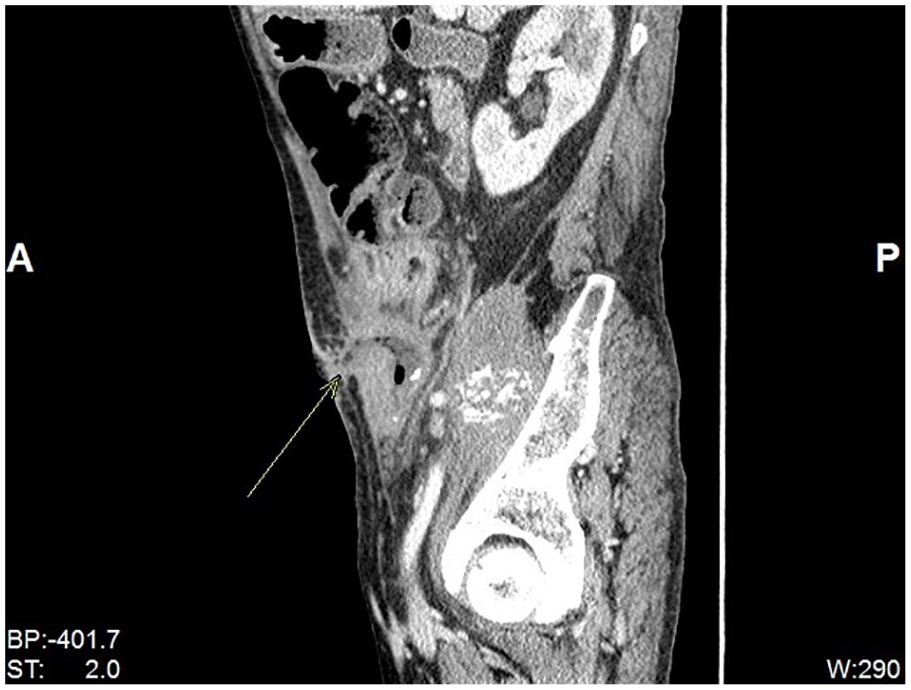
Sagittal reconstruction of CT Abdomen and Pelvis with oral and IV contrast showing enterocutaneous fistula.
Discussion
CRC is the third most common malignancy and the second most common deadly cancer worldwide as of 2020. 1 Based on cancer statistics data, approximately 1 in 23 males and 1 in 25 females in the United States will be diagnosed with CRC during their lifetime. 2 The usual presenting complaints of CRC are altered bowel habits, per-rectal bleeding, and abdominal discomfort. Unusual symptoms at presentation may be noted when the cancer is locally advanced and locally advanced cases without distant metastases are rare, accounting for 5% to 22% of all CRC. 3 Direct invasion of tumor cells along the tissue planes may result in the formation of phlegmon/abscess in the abdominal wall musculature as in our case. There are only a few case reports of abdominal wall involvement by CRC as the initial presentation.4-6 White et al 7 reviewed 16 000 colon cancer patients at Massachusetts General Hospital between 1938 and 1970, out of which only 9 had a presenting complaint of abdominal wall abscess.
Our case is unique not only because of its uncommon presentation but also due to its aggressive course. It is unusual for surgically operated CRC with negative margins to progress on intensive FOLFOX therapy. Cytoreductive surgery (CRS) followed by HIPEC was undertaken in this case as it is proven to significantly add survival time for patients with peritoneal carcinomatosis due to CRC. 8 Adjuvant systemic chemotherapy when compared with active surveillance was associated with improved median overall survival following CRS and HIPEC. 9 FOLFIRI was selected as the adjuvant regimen as patient initially failed to respond to FOLFOX. Pooled analysis of data from 7 clinical trials involving advanced CRC patients demonstrated an increased median survival with administration of all 3 cytotoxic agents—5-fluorouracil, oxaliplatin, and irinotecan—at some point in the treatment course. 10 Postoperative radiotherapy is not a routine component of care for colon cancers unlike rectal cancers. However, it was given in our case as it is shown that high-risk CRC cases with associated abscess or fistula formation may benefit from adjuvant radiotherapy in addition to systemic therapy. 11 Third-line therapy with trifluridine/tipiracil and bevacizumab was subsequently chosen for this patient as the tumor was refractory to standard therapies. This combination had a clinically significant and relevant improvement in progression-free survival with manageable toxicities in chemorefractory-advanced CRC cases. 12 Despite all the above management, cure could not be achieved in this case and cancer continued to progress leading to development of an enterocutaneous fistula. On the grounds of poor quality of life, patient decided on hospice care.
In the current era of ongoing tremendous developments in colorectal cancer diagnosis and treatment, this uncommon case reminds us that locally advanced CRC is still a challenge. Precision medicine with treatment strategies tailored to an individual’s genetic, environmental, and lifestyle factors is the current need. Extended genetic testing with gene-targeted therapies may be instrumental in salvaging patients who are unresponsive to conventional therapies. This case also emphasizes the need for timely CRC screening as our patient never had a screening colonoscopy. The importance of screening in early diagnosis of CRC cannot be stressed enough. Depending on a patient’s personal and familial risk factors, CRC screening at appropriate times should be undertaken during routine health care visits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.