
Abstract
Paratesticular rhabdomyosarcoma (RMS) is a rare malignancy, representing ~3% of all pediatric soft tissue tumors. The spindle cell subtype, a variant of embryonal RMS, is particularly uncommon but is typically associated with a favorable prognosis. We report the case of a 12-year-old boy who presented with a painless, progressively enlarging right inguinoscrotal mass. Imaging studies revealed a heterogeneous lesion without distant metastasis, and tumor markers were within normal limits. The patient underwent radical orchiectomy, and histopathology confirmed spindle cell RMS, with immunohistochemical positivity for myogenin and desmin. After completing treatment with the Children’s Oncology Group (COG)-ARST0531 Vincristine, Actinomycin D, and Cyclophosphamide protocol, a retroperitoneal lymph node recurrence was detected 1 year later. Management consisted of surgical resection and escalated chemotherapy per the COG-ARST0431 protocol, with subsequent imaging showing no evidence of disease. This case demonstrates that despite a favorable histology, paratesticular spindle cell RMS carries a risk of late, regional recurrence, underscoring the necessity of vigilant long-term surveillance. We also performed a systematic literature review to contextualize our findings, focusing on clinical presentation, therapeutic strategies, and outcomes.
Introduction
Rhabdomyosarcoma (RMS) is a rare malignancy that originates from primitive mesenchymal cells, 1 accounting for ~3% of all pediatric tumors. 2 The incidence of RMS follows a bimodal age distribution, with an initial peak between the ages of 2 and 5 and a second peak in adolescents under 20 years old. 3
The tumor typically metastasizes through the lymphatic system to the iliac and para-aortic lymph nodes. Distant metastases most frequently occur in the lungs, bones, and bone marrow. 4 Paratesticular RMS arises from the diverse, non-testicular structures within the scrotum, such as the epididymis, spermatic cord, tunica vaginalis, and other associated supportive tissues. 5
Histopathological examination of the spindle cell subtype of RMS is characterized by the proliferation of spindle-shaped cells arranged in fascicles or whorls. 6 The standard management of RMS is multimodal and combines surgical intervention, chemotherapy, and radiation therapy to optimize treatment outcomes and reduce the risk of recurrence. 7 This article presents a rare case of pediatric paratesticular spindle cell RMS, supplemented with a systematic review to evaluate current diagnostic and therapeutic standards.
Case Presentation
A 12-year-old male with an unremarkable past medical and family history presented to our hospital with a chief complaint of a painless swelling in the right inguinoscrotal area, which had been progressively increasing in size over the preceding 2 months. On physical examination, a firm, nontender mass was palpated in the right hemiscrotum. There was no transillumination or an associated cough impulse. Initial laboratory investigations, including serum tumor markers alpha-fetoprotein (AFP), beta-human chorionic gonadotropin (β-hCG), and lactate dehydrogenase, were unremarkable and within normal limits. A diagnostic imaging workup was initiated. Scrotal ultrasonography demonstrated an ill-defined, heterogeneous lesion measuring ~8 × 4 cm in the right hemiscrotum, which exhibited internal vascularity and was displacing the right testis (Figure 1). Subsequent magnetic resonance imaging (MRI) of the pelvis characterized the lesion as a heterogeneously enhancing mass. Staging with chest and abdominal MRI revealed no evidence of metastatic disease (Figure 2). Based on the clinical and imaging findings, the patient underwent a right radical orchiectomy. The surgical specimen was sent for histopathological analysis, which confirmed a diagnosis of spindle cell RMS. The diagnosis was further supported by immunohistochemistry, which showed the tumor cells were positive for myogenin and desmin, consistent with skeletal muscle differentiation (Figure 3). A postoperative computed tomography (CT) scan of the pelvis with IV contrast showed expected postsurgical changes with no signs of a residual mass (Figure 4). Following the definitive diagnosis and staging, the patient was started on systemic chemotherapy according to the Children’s Oncology Group (COG)-ARST0531 VAC protocol, consisting of Vincristine (1.5 mg/m2), actinomycin D (0.045 mg/kg), and cyclophosphamide (1200 mg/m2). The patient completed all planned cycles of chemotherapy over 6 months. He then entered a surveillance phase with imaging conducted every 3 months. At the 12-month follow-up, a routine surveillance CT scan revealed new retroperitoneal lymphadenopathy, consistent with recurrence (Figure 5). The patient then underwent a retroperitoneal lymph node dissection, with an excisional biopsy confirming metastatic spindle cell sarcoma. Consequently, his treatment was escalated according to the COG-ARST0431 protocol.

Scrotal ultrasonography. B-mode (A) and color Doppler (B) images demonstrate a large, heterogeneous paratesticular mass (green arrow) with internal vascularity (red arrow). The mass displaces the right testis, which contains a focal heterogeneous area (yellow arrow).

Pelvic MRI. Multiplanar images characterize the paratesticular mass (green arrow). The lesion is hypointense on the T1-weighted image (A), hyperintense on the T2-weighted image (B), and shows intense, heterogeneous enhancement after contrast administration (C, D). The mass displaces the right testis (blue arrow). Note the undescended left testis in the inguinal canal (red arrow). MRI, magnetic resonance imaging.

Histopathology and IHC. (A) Proliferation of spindle cells arranged in fascicles (H&E stain, 10× magnification). (B) At higher power, the cells show nuclear pleomorphism and high mitotic activity (H&E stain, 20× magnification). (C) Tumor cells demonstrate positive immunostaining for myogenin and desmin (IHC, 20× magnification). IHC, immunohistochemistry.
Postoperative pelvic CT scan. Axial CT with intravenous contrast shows expected postoperative changes, including fibrotic stranding in the surgical bed (blue arrow). CT, computed tomography.

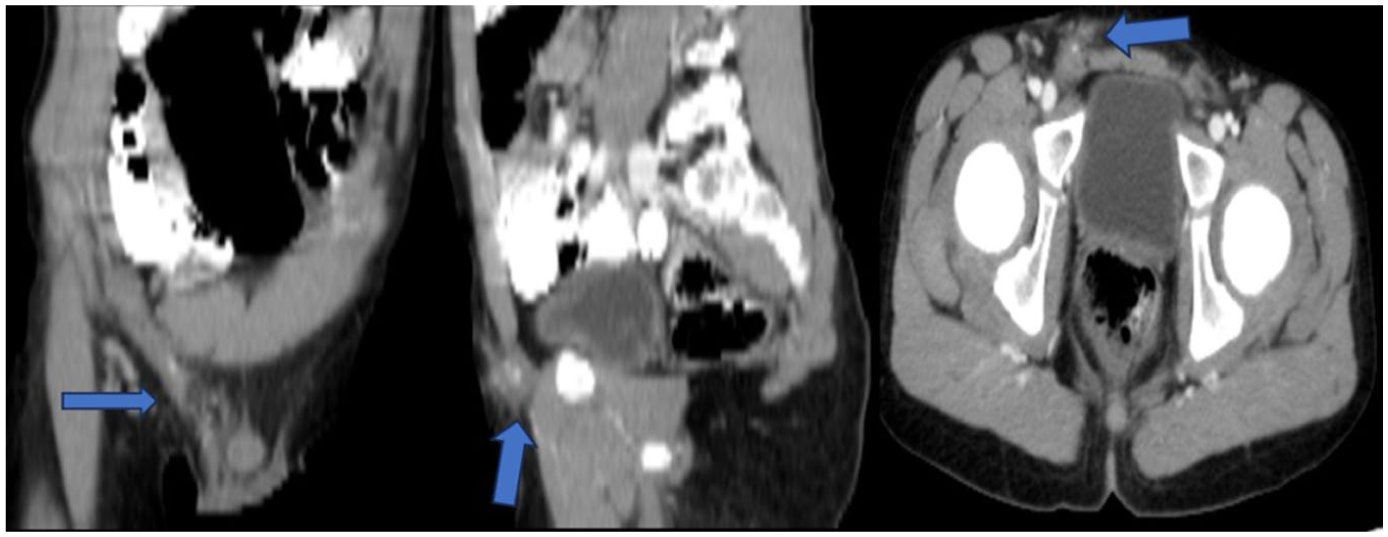
Surveillance CT scan showing recurrence. Follow-up axial CT scan at 12 months reveals a new, enhancing retroperitoneal lymph node (blue arrow) in the aortocaval space, consistent with disease recurrence. CT, computed tomography.
Postsurgery and subsequent chemotherapy, follow-up positron emission tomography scans have shown no evidence of local recurrence or distant metastases. The patient is currently in good health, attending school, and remains under regular clinical and radiological surveillance.
Discussion
This case of pediatric paratesticular spindle cell RMS is notable for its retroperitoneal recurrence 1 year after initial therapy, a development that occurred despite the favorable prognosis typically associated with this histology. This outcome underscores the critical need for vigilant surveillance and highlights key aspects of the disease’s diagnosis, management, and metastatic potential.
Histological Subtype and Prognosis
RMS has several histological forms, including alveolar, pleomorphic, and embryonal. 4 Spindle cell RMS, a recognized embryonal subtype, is uncommon and represents only about 5% of all RMS cases. 8 It is distinguished by the fascicular growth of spindle-shaped cells that exhibit rhabdomyoblastic differentiation, a finding that was confirmed in our patient’s pathological specimen. This RMS subtype shows a significant male predominance, with a reported ratio of 6:1 compared to females, which aligns with our case. 9
While paratesticular spindle cell RMS is often cited for its favorable prognosis compared to other subtypes, our case challenges this generalization. 10 The development of retroperitoneal recurrence 1 year after standard therapy illustrates that clinical outcomes are critically dependent on factors beyond histology, including the completeness of surgical excision and the potential for occult micrometastatic disease. 10
Key factors influencing prognosis include patient age, tumor location and size, the success of surgical excision, and the presence of metastatic spread. While patients with localized disease often have high survival rates, those with lymph node involvement or distant metastases face increased recurrence risks. The presence of residual tumor postsurgery significantly affects long-term prognosis, highlighting the importance of complete removal followed by appropriate chemotherapy. 11
Diagnostic Approach: Imaging, Tumor Markers, and Pathology
When evaluating a patient with a mass in the scrotal or inguinal area, a thorough physical examination and a full medical history are the initial assessments. 12 The tumor typically appears as a firm, nonpainful swelling in the inguinoscrotal region; its dimensions and growth duration can differ, and it rarely penetrates the scrotal skin. 1 Ultrasonography is the primary diagnostic tool used initially. It can identify the lesion as a hypoechoic image and evaluate its vascularity through Doppler imaging, which often shows an increase, as was observed in our patient. 13
In RMS, tumor markers such as AFP, β-hCG, and carcinoembryonic antigen are typically not elevated and remain within normal reference ranges, a finding that was also consistent with our patient’s presentation. 4 Tumor cells frequently interact with myogenic markers such as myf-4 (myogenin), desmin, titin, troponin D, myoglobin, and MyoD1. 14 Our patient’s immunohistochemical analysis confirmed this, showing positivity for myogenin and desmin.
Although some studies suggest that about 25% of paratesticular RMS cases involve retroperitoneal lymph nodes, our review of published case reports found limited direct evidence of this. This suggests a potential gap in case reporting and emphasizes the need for thorough imaging during staging. 15 The development of recurrence in our patient, despite adherence to a standard protocol, reinforces that the risk of lymphatic spread remains a significant clinical concern even in subtypes with a favorable prognosis.
Treatment Modalities and the Role of Surveillance
The management of paratesticular RMS is multidisciplinary, involving radical orchiectomy, adjuvant chemotherapy, and sometimes radiation therapy. Our patient was treated according to standard COG protocols, initially with VAC chemotherapy. The development of a retroperitoneal recurrence at the 12-month follow-up, despite adherence to this standard protocol, is the most clinically significant aspect of this case. This event highlights the limitations of initial staging sensitivity in detecting micrometastatic disease and reinforces that the risk of lymphatic spread remains a significant clinical concern. This prompted an escalation of therapy, which successfully controlled the disease.15,16
Insights From the Systematic Literature Review
To better understand the clinical features, diagnostic approaches, and outcomes of this disease, we conducted a systematic literature review using the PubMed database. We used the following search strategy: (“spindle cell rhabdomyosarcoma” AND “case” AND “paratesticular”) with no date or language restrictions. Articles were screened manually, and only individual case reports with sufficient clinical detail and confirmed histopathology were included for analysis. The cases summarized in Table 1, which were yielded from our systematic review, provide critical context for the management and outcome of our 12-year-old patient. The literature confirms the known male predominance, a finding consistent with our case. The patient age in the reviewed cases spans from adolescence to late adulthood, highlighting that while our patient falls within the typical pediatric demographic, this is not exclusively a pediatric disease. Tumor size at diagnosis varied significantly, from 3 cm to a massive 25 cm.Our analysis of 13 published cases reveals a more aggressive potential than the “favorable prognosis” label suggests. Of the cases with follow-up data, 6 (46%) had lymph node involvement either at diagnosis or during follow-up and 4 (31%) experienced disease recurrence or progression. Our patient’s clinical course is particularly instructive: he initially presented with localized disease (Stage 1, Group I) but later declared himself to have had occult metastatic disease by developing a retroperitoneal recurrence. This case serves as a crucial bridge between patients with truly localized disease and those presenting with overt metastases. It demonstrates that initial negative staging does not preclude the risk of lymphatic spread and reinforces the idea that vigilant surveillance of the retroperitoneal lymph nodes is not merely precautionary, but essential. This review highlights key prognostic factors that appear to predict worse outcomes. Specifically, large tumor size (such as the 25 cm mass reported by Silvestris et al) and the presence of nodal involvement at diagnosis (Dey et al 18 and Nascimento et al 19 ) were associated with widespread metastatic disease and poor outcomes, suggesting that a larger tumor burden may correlate with more aggressive biology.
Summary of Published Cases of Paratesticular Spindle Cell RMS.

Abbreviations: AFP, alpha-fetoprotein; β-hCG, beta-human chorionic gonadotropin; CECT, contrast-enhanced computed tomography; CT, computed tomography; DIC, disseminated intravascular coagulation; FNA, fine needle aspiration; IHC, immunohistochemistry; LDH, lactate dehydrogenase; MRI, magnetic resonance imaging; NK, not known; RA-RPLND, robot-assisted retroperitoneal lymph node dissection; RMS, rhabdomyosarcoma; RPLND, retroperitoneal lymph node dissection; US, ultrasonography; VAC, Vincristine, Actinomycin D, and Cyclophosphamide.
This is another excellent case series by Rekhi and Singhvi. 17 It includes 21 cases of spindle cell/sclerosing RMS, but only 2 of them are paratesticular.
The most critical insight from this analysis, however, relates to metastatic potential and prognosis, which directly informs the key event in our patient’s journey his retroperitoneal recurrence. While our patient initially presented with clinically localized disease (negative staging), the subsequent development of retroperitoneal recurrence at 1 year demonstrates that initial imaging can fail to detect micrometastatic disease. Our patient’s development of a retroperitoneal recurrence after presenting with clinically localized disease directly reflects this risk, unmasking what was likely occult metastatic disease from the start. This is mirrored by the case from Nascimento et al, where an 18-year-old presented with 10 positive lymph nodes, further underscoring the high potential for early lymphatic spread. The poor outcomes in patients with nodal involvement (Dey et al, 18 Nascimento et al, 19 and Silvestris et al 20 ) contrast sharply with the more favorable outcomes in those with truly localized disease. This case illustrates that apparent clinical localization at diagnosis does not exclude the presence of occult metastatic disease. It highlights the need for improved staging sensitivity and long-term surveillance. Therefore, our case serves as a crucial bridge between these 2 groups: it proves that a patient who appears to have localized disease at diagnosis can later declare themselves as having had occult metastatic disease all along. This strongly supports the argument for aggressive management and validates our decision to escalate treatment following the detection of his recurrence. This review, therefore, compellingly refutes any notion of a uniformly benign prognosis and emphasizes that vigilant, long-term surveillance of the retroperitoneal lymph nodes is essential for all patients, as initial staging may be insufficient to detect micrometastatic disease.
Conclusion
Paratesticular spindle cell RMS is a rare tumor that, while often associated with a favorable prognosis, can exhibit aggressive behavior, as demonstrated by the regional recurrence in our patient. This case underscores that early diagnosis, achieved through a combination of radiological imaging and definitive immunohistochemical analysis, is critical for successful management. The primary treatment strategy remains complete surgical excision with adjuvant, protocol-based chemotherapy. Most importantly, this case serves as a crucial reminder that even in prognostically favorable subtypes of RMS, the risk of late regional recurrence is significant. This case demonstrates that rigorous, long-term surveillance is essential. For our patient, it was the critical factor that allowed for the timely detection and treatment of his recurrence, leading to a positive outcome.
Footnotes
Acknowledgements
The authors extend their heartfelt gratitude to the patient’s family for their cooperation and consent. They also express appreciation to the Polytechnic Medical Students’ Research Association (PMRA) for their logistical and technical assistance.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient’s legally authorized representative for participation in this study and the publication of this case report.
Consent for Publication
Written informed consent was obtained from the patient’s legally authorized representative for the publication of this case report and any accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.