
Abstract
Chronic diarrhea is a common reason for consultation in renal transplant patients. Cytomegalovirus infection is the cause of chronic diarrhea of infectious origin in 50% of cases, but coinfection with tuberculosis is rare. We present the case of a renal transplant patient with chronic diarrhea, with a finding of left colon colitis and positive microbiological studies in biopsy for tuberculosis and cytomegalovirus. The patient received valganciclovir and anti-tubercular treatment with adequate evolution. Immunosuppressed patients may have diarrhea secondary to opportunistic infections; therefore, an algorithm for early diagnosis and treatment is recommended.
Introduction
Chronic diarrhea is a common reason for consultation in renal transplant (RT) patients. The most common causes are immunosuppressive agents, infections, and antibiotics. 1
The incidence of post-transplant (PostTx) diarrhea ranges from 11.5% to 22.6% in the first 3 years after transplantation. 1
Among the infectious causes, up to 50% of cases of diarrhea in PostTx patients are due to cytomegalovirus (CMV) infection. 1 On the contrary, the prevalence of tuberculosis (TB) in RT is lower, reported to be between 0.3% and 1.7%. 2 Gastrointestinal tuberculosis (GITB) in RT is a rare but potentially fatal presentation that should be suspected in all immunosuppressed patients with chronic diarrhea.
Case Report
The case is a 32-year-old female patient with a history of cadaveric donor RT in 2006 due to membranoproliferative glomerulonephritis. She received induction therapy with basiliximab and maintenance therapy with tacrolimus, mycophenolate, and deflazacort. She consulted for a 4-week history of diarrheal stools 4 times a day that she controlled with loperamide. In the last week, it was associated with nausea, crampy abdominal pain, and fever. In the last 6 months, she had lost 10 kg and was being managed with oral iron due to normochromic normocytic anemia, with no improvement in hemoglobin levels. She had no other relevant background.
On physical examination, she was tachycardic, afebrile, and normotensive, with abdominal pain in the left flank without signs of peritoneal irritation. Chronic diarrhea and febrile syndrome were considered in an immunosuppressed patient, so studies with fecal microscopy, fecal culture, viral load for CMV, and blood culture were started (Table 1). Due to chronic anemia, studies with folic acid, vitamin B12, ferrokinetic profile, and nutritional profile were extended, confirming iron deficiency anemia.
Admission Laboratories.

Renal function was stable with serum creatinine within the patient’s usual range. Electrolytes were unaltered, fecal microscopy examination was inflammatory, and cultures were negative. Colonoscopy showed left and transverse colitis with 80% stenosis of the colonic lumen (Figure 1). Biopsies of the compromised segments were taken.
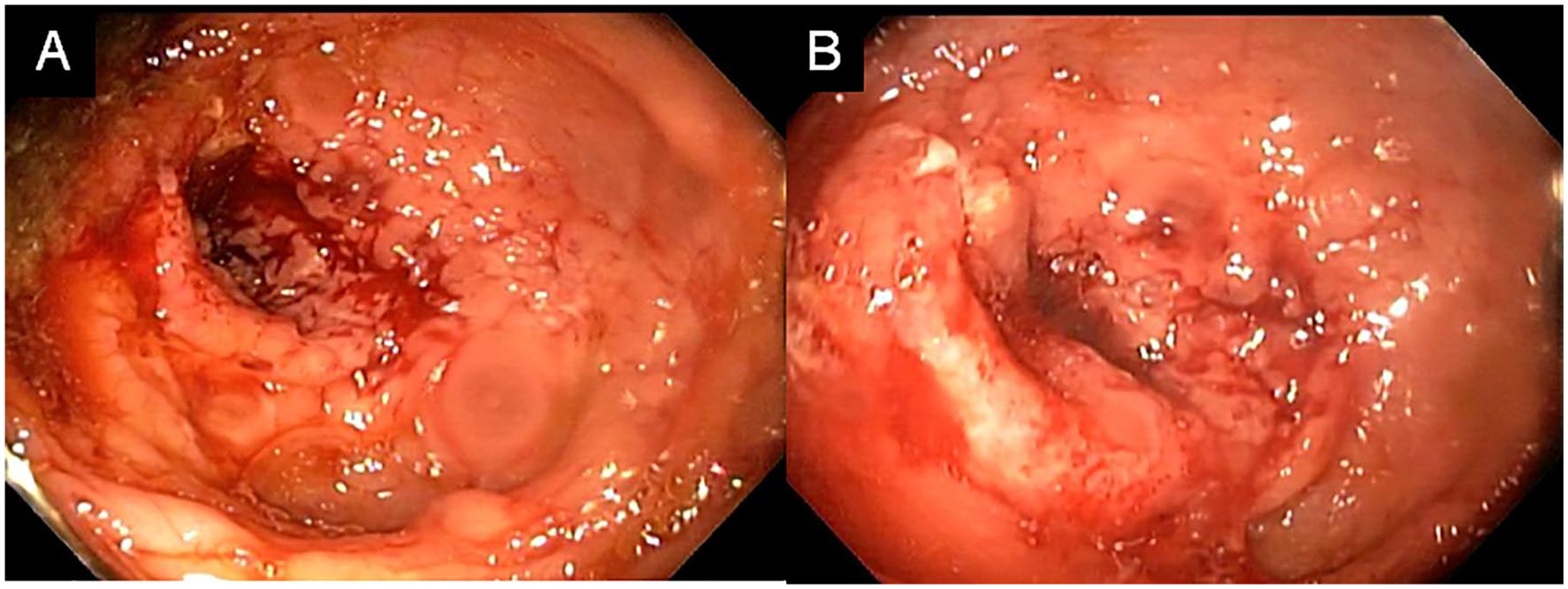
Colonoscopy. (A) Left and transverse colitis with 80% stenosis of the lumen. (B) Areas of thickened mucosa, irregular cobblestone appearance, ulcerated, easy bleeding, and stenotic segments with loss of vascular pattern.
Given the results found in colonoscopy, studies with gastrointestinal film array, CMV viral load in plasma, HIV, and rapid plasma reagin were evaluated, which were negative, as was the Histoplasma urine antigen. Herpes simplex type I and II studies performed in biopsy were negative. Given the suspicion of neoplasia, contrast abdominal tomography was carried out, which showed thickening and enhancement of the walls of the cecum, ascending colon, and hepatic flexure of the colon, with a 4-cm segment with 80% stenosis of the ascending colon lumen. Colon biopsy reported ulcerative component, without identifying microorganisms, dysplasia, or malignancy. Polymerase chain reaction (PCR) for TB and CMV was positive in the biopsy.
The patient was presented at a meeting considering intestinal Mycobacterium tuberculosis (MT) and CMV coinfection. Treatment with valganciclovir for 4 weeks was decided to manage CMV and 4-drug therapy with isoniazid (INH), rifampin (R), pyrazinamide (Z), ethambutol (E), and pyridoxine for GITB management. Tacrolimus dose was adjusted due to drug interaction with rifampin.
During treatment, elevated transaminases (aspartate aminotransferase 414 U/L and alanine transaminase 990 U/L) and uric acid (16 mg/dL) developed. Hepatotoxicity associated with INH was considered, so it was assessed by the pulmonologist who changed INH to moxifloxacin, with improvement in the liver profile. Moxifloxacin, R, and Z were continued for 9 months. The evolution was satisfactory, with the resolution of diarrhea, improvement in anemia, stable renal function (1.48 mg/dL), and weight recovery.
Discussion
In the PostTx state, the incidence of diarrhea varies by year post-transplant, increasing with each year, being higher in the third year, with reports of up to 22% cumulative incidence. 1 Bunnapradist et al 2 reported that PostTx diarrhea doubled the risk of patient death and graft loss. Post-transplant diarrhea is associated with complications such as acute kidney injury and the need to reduce immunosuppressive agents’ dose, increasing mortality or graft loss risk. 3
As in immunocompetent patients, most episodes of diarrhea in PostTx patients are self-limited and have no identifiable cause. Among the identifiable causes, the most important are infections, immunosuppressive agents, and antibiotics. In infectious causes, those generated by Clostridium difficile, norovirus, and CMV 4 stand out. In the prospective study Diarrhea Diagnosis Aid and Clinical Treatment (DIDACT), 5 an infectious cause was identified in 28% of patients, with Campylobacter jejuni and CMV being the most common. However, the etiological agent varies according to each region. For example, in a study by Shad et al 6 in Pakistan, the most common infectious cause was Giardia lamblia (29%), and the least common was tropical sprue with 7%. Tuberculosis ranked fourth with 11%.
Mycobacterium tuberculosis is a common infectious agent in developing countries. In transplant patients, the incidence is more frequent, with 512 cases/100 inhabitants/year, and can be caused by primary infection, reactivation of latent TB favored by immunosuppression, or to a lesser extent (4%), it can be transmitted by the graft. 7 Reactivation is 20 to 74 times more frequent in solid organ transplant recipients than in the general population. 7
Post-transplant renal TB prevalence is reported to be between 0.3% and 1.7%. 8 Singh and Paterson 8 found that the mean time of TB onset in patients with RT was 11.5 months. Most cases are due to latent infection reactivation and usually involve the lungs. However, in RT, extrapulmonary disease (15%) and disseminated TB (33%-49%) are common. 9 The classic presentation is not usual in these patients; therefore, the typical clinical picture is not what leads to the diagnosis but rather the clinical suspicion.
Among the manifestations of RT TB, GIBT is an unusual presentation but can lead to death. The prevalence in PostTx renal patients is close to 0.5% (especially in low-income countries), exponentially higher than in immunocompetent people. 10 The main risk factors are high doses of immunosuppression and the first year PostTx (period where approximately 60% of cases occur). 11
The symptoms that should be looked for in patients with suspected GITB in this type of patients are intestinal bleeding, fever, and abdominal pain because these are the most common and are associated with an ulcerative presentation of the disease, as occurred in this case. Intestinal obstruction is extremely rare, with an indolent course being more frequent. 12
In imaging studies, it is common to find a nodular or ulcerated appearance of the mucosa, predominantly in the terminal ileum. The most common finding on computed tomography is intestinal mural thickening, although it can also show loop inflammation and ascites. 13 The ileocecal region, jejunum, and ileum are involved in 75% of cases of TBGI. 13
Diagnosis of TB can be difficult because it depends on the identification of MT. Traditional methods such as direct microbiological examination have low sensitivity, and culture reporting is delayed (up to 6 weeks). 14 Another option is Xpert MTB/RIF PCR, which has a sensitivity of 66%, a specificity of 100%, a negative predictive value of 93.3, and a positive predictive value of 100. 15 Endoscopic findings should be taken into account, such as the presence of ulcers, small diverticula, sessile polyps, nodules, and mucosal strictures. 16
For the diagnosis of gastrointestinal CMV infection, studies such as viral load or antigen detection by PCR are used, with a sensitivity and specificity for the pp65 antigen assay of 94% and 99%, respectively. 17 However, these tests may be negative. The gold standard is evidence of cytopathic changes in tissue samples. 18
Anti-TB treatment for these patients is the same as used in the general population, comprising the administration of INH, R, Z, and E for 2 months, followed by INH and R for a minimum of 4 months. 19 The time to start treatment depends on the degree of diagnostic suspicion; when it is high, it can be empirical, even when Mycobacterium tuberculosis is not isolated. Calcineurin inhibitor monitoring and adjustment are necessary to avoid graft rejection and toxicity.
In patients with RT, the mortality associated with GITB varies between 20% and 30%. 20 About half of the deaths are due to sepsis within the first 3 months of diarrhea onset. There are few reported cases in the literature of GITB in PostTx patients. A rigorous diagnostic approach is necessary to allow early diagnosis and timely treatment.
The case patient is currently asymptomatic, without gastrointestinal symptoms and with stable renal function.
Footnotes
Acknowledgements
The authors acknowledge Dr Daniela CácSaneres Escobar and Andrés Ardila for the images taken from the colonoscopy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Institutional Ethics Committee (approval number FM-CIE-1225-21).
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.