
Abstract
Cryptococcal meningitis (CM), as a life-threatening opportunistic infection, often is among cases with cell-mediated immunodeficiencies, such as AIDS, hematologic malignancies, and solid organ transplant recipients. Cryptococcal meningitis in healthy individuals is uncommon, and its detection in immunocompetent cases may be tricky because the presentation is generally more indolent than the traditional meningitis presentation, leading to late diagnosis and potential sequels. We present a CM case in an immunocompetent Iranian male patient who was treated successfully.
Introduction
Cryptococcal meningitis (CM), a serious fungal infection due to encapsulated saprophytic yeast, either Cryptococcus neoformans or Cryptococcus gattii, is seen increasingly in cases with late-stage HIV or other forms of cell-mediated immunodeficiency, including patients receiving immunosuppressive drugs and solid organ transplant recipients. Mortality of HIV-associated CM, despite therapy, remains high, that is, 10% to 30%; however, its mortality in low-income countries may exceed even up to 70%.1,2 The development of CM in immunocompetent patients is relatively rare, although the latest reports of these cases are growing. 3 We here report a CM case in an apparently immunocompetent 55-year-old Iranian male patient who was treated with favorable outcome.
Case Presentation
A 55-year-old man was referred to the emergency department with a 20-day history of gradual onset of headache. He had presented to another emergency department over this period with a persistent severe headache, being prescribed analgesics; however, no significant improvement was observed. His headache was generalized and accompanied by vomiting and nausea. He was a non-diabetic normotensive patient without other medical or surgical history with no medications. He was alert, afebrile, and hemodynamically stable at admission. He had a blood pressure of 120/70 mm Hg, heart rate of 87 beats per min, respiratory rate of 18 breaths per min, and SpO2 of 95%—room air. His pupils were identical and responsive to light, and his cranial nerves, motor, and sensory systems were normal. Kernig and Brudzinski’s signs were also negative. The rest of the physical examination was normal. The blood count exhibited a leukocyte amount of 8800 cells/µl (with differential cell count being normal), hemoglobin of 13 g/dL, and also a platelet amount of 334 000 platelets/µL. Liver enzymes, renal function tests, serum electrolytes, and blood glucose were within normal limits. The findings of initial brain magnetic resonance imaging revealed no abnormality.
Lumbar puncture results included normal initial pressure with semi-clear cerebrospinal fluid (CSF). According to CSF examination, there were 300 white blood cells/mm3, among which 10% were poly-morphs and 90% mono-morphs; adenosine deaminase of 14 U/L (normal range in CSF: up to 9); sugar of 55 mg/dL; protein of 35 mg/dL; and angiotensin-converting enzyme of 1 IU/L (normal range: up to 9). CSF Venereal Disease Research Laboratory and Wright were negative. No acid-fast bacilli were seen in staining. Gram staining of CSF sample revealed budding yeast cells (Figure 1). The CSF culture was negative for bacteria and mycobacterium species. Mycobacterium tuberculosis polymerase chain reaction (PCR) and also PCR fungal panel were all negative with the exception of Cryptococcus neoformans. The CSF for cytopathology revealed no evidence for malignant cells.
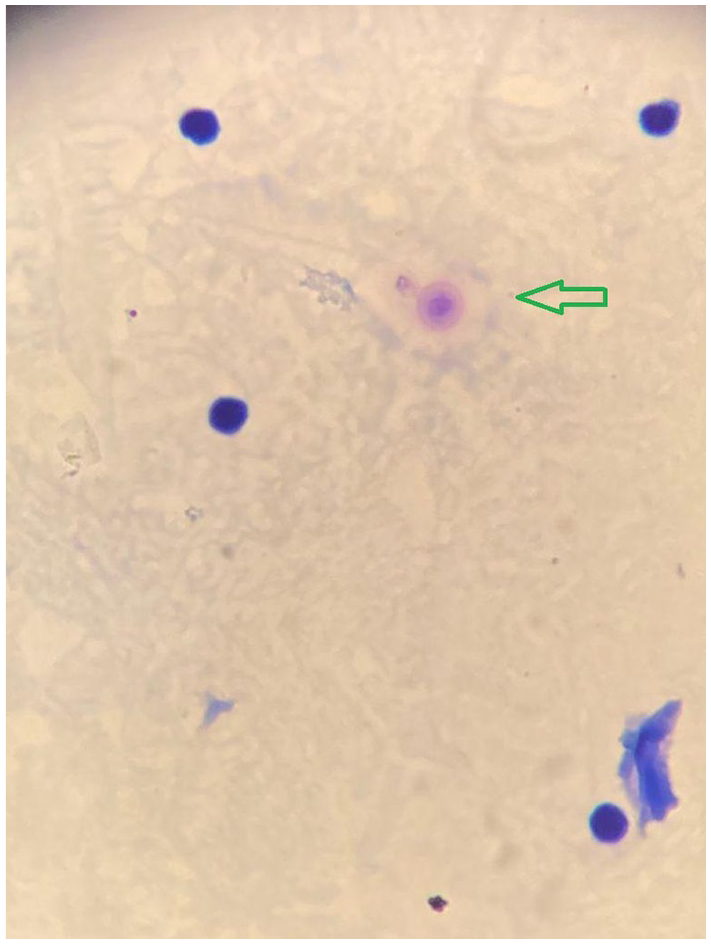
Gram staining of the cerebrospinal fluid sample revealed budding, thin-walled, cells containing gram-positive granular inclusions, surrounded by a capsule compatible with encapsulated yeast form (green arrow).
According to the laboratory data, the diagnosis of CM caused by C neoformans was made, and liposomal amphotericin B (5 mg/kg/day) accompanied by fluconazole (800 mg/day) was initiated. Once 2-week course of antifungal therapy was done, the patient was well with no headache and was subsequently discharged on fluconazole (800 mg/day) for 8 weeks. He was then started on fluconazole (400 mg/day) after completing 8 weeks of therapy. The tests of serum HIV antibodies using enzyme-linked immunosorbent assay (ELISA) several times were negative. Absolute neutrophil count (ANC), total lymphocyte count (TLC), and immunoelectrophoresis-serum test were normal. Also, the tuberculin skin test was negative. Two-month follow-up showed that he is healthy with no residual neurological sequelae.
Discussion
Cryptococcal infection is a life-threatening opportunistic infection, and most cases are in those with cell-mediated immunodeficiency, including AIDS particularly when their CD4 drops under 100 cells/μL, solid organ transplant recipients, and in those with hematologic malignancies; however, this infection is infrequent after hematopoietic stem cell transplantation1,4,5 Several states, including diabetes mellitus, alcoholism, and also cirrhosis, may precipitate mild states of immunosuppression, potentially predisposing hosts to cryptococcal infection. 6 The disease’s most common clinical manifestation affecting the central nervous system (CNS) in immunocompromised patients is meningoencephalitis or meningitis, with high mortality rate. Another CNS manifestation is cryptococcomas, which are mass lesions with focal tissue infection establishment. A cryptococcoma formation depends on an inflammatory process; hence, this entity is more frequently observed in immunocompetent people and is more prevalent with C gattii rather than C neoformans. Pulmonary, cutaneous, and other organ involvement can occur due to cryptococcemia.7-9
The most common symptom of CM is headache with or without decreased level of consciousness. In the majority of cases, intracranial pressure (ICP) is often high, causing consequent cranial nerve palsies or seizures. Meningism features, including neck stiffness, happen in fewer than 20% of cases. 10 If treatment is not initiated on time, the infection may lead to seizures, confusion, decreased consciousness level, and finally coma with poor prognosis. 11
In healthy people, CM is relatively rare, even though its latest reports are growing. In evaluation of these patients, some etiologies for immunosuppression are defined. The best-recognized risk factor in such patients is idiopathic CD4 T-lymphocytopenia, a heterogeneous disease with an uncertain origin. 12 Pulmonary alveolar proteinosis and autoantibodies against interferon-γ has also been related to intracellular infections, including cryptococcosis.13,14 The essential role of GATA2 zinc finger transcription in lymphatic vascular development, lymphatic angiogenesis, and also morphogenesis of lymphovenous and lymphatic vessel valves is well defined. 15 It is described that mutations in GATA2 have been associated with cryptococcosis. 16 Some studies highlighted the susceptibility of X-linked hyper-IgM syndrome and also hyper-IgE syndrome patients to cryptococcosis.17,18
Acharya et al 19 reported a 59-year-old man hospitalized with confusion and irrelevant speech with the diagnosis of CM and treated with favorable outcome. Murphy et al 20 described an immunocompetent 35-year-old man who presented with a chronic severe headache and was diagnosed with CM, which resulted in a lengthy hospitalization and considerable neurologic decline. Khattab et al 21 described a 53-year-old Caucasian male who presented with a history of 2-week severe bilateral eye pain and diplopia.
In this article, we present a case of Iranian man who was admitted with a history of persistent headache, and after evaluation of CSF, including Gram staining and PCR, the diagnosis of CM was made and improved with antifungal therapy. The tests of serum HIV antibodies using ELISA several times were negative. Also, ANC, TLC, and immunoelectrophoresis-serum test were normal. The tuberculin skin test was negative; hence, the CM diagnosis in an apparent immunocompetent patient was established. The favorable outcome of this case may be accredited to early diagnosis, rapid initiation of appropriate antifungal therapy, and also the absence of any complications such as fungemia or raised ICP.
Disease recognition in immunocompetent cases may be hard, and its presentation is mostly more indolent than classical meningitis presentation, leading to late diagnosis and consequent sequels. Cryptococcal meningitis management, including antifungal regimens, early detection, and treatment of raised ICP and diagnosis of immune reconstitution inflammatory syndrome, was done. The standard induction treatment is 2 weeks of amphotericin B plus flucytosine, 22 but the treatment in resource-limited setting is challenging and flucytosine is not available in many countries; therefore, many rely on monotherapy with amphotericin B with or without combination of fluconazole for induction therapy. 23 In this case, liposomal amphotericin B and fluconazole combination was used for induction therapy owing to flucytosine unavailability in Iran. At the end of the second week, he was discharged on fluconazole as the consolidation therapy.
In CM, delayed diagnosis due to the subacute nature of symptoms can occur. High clinical suspicions must be considered, and using accessible diagnostic modalities may serve early diagnosis and avoid morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Individual cases or case series do not require ethical approval at our institution.
Informed Consent
The patient provided written informed consent for his anonymized information to be published in this research.