
Abstract
Infection of the thyroid gland with Coccidioides immitis is rare. We report a case with disseminated coccidiomycosis involving thyroid gland as a thyroid nodule. Although historical autopsy studies have indicated that coccidioidal involvement of the thyroid gland can infrequently occur as part of disseminated infection, to our knowledge, only less than 10 other cases have been reported. Optimal treatment duration and dosage of medication are uncertain in literature of this rare involvement of thyroid gland with coccidioidomycosis.
Purpose of Study
Coccidioidomycosis is endemic to the Southwestern United States and Northern Mexico. Most patients have primary Coccidioidomycosis with pulmonary involvement. Dissemination to the thyroid gland is rare, with less than 10 cases reported in the English literature since 1979.
Methods Used
This is a retrospective review of medical records at Kern Medical. The search engines used were PubMed search, UpToDate search, and Google scholar.
Summary of Results
A 53-year-old Latinx woman with past medical history of poorly controlled diabetes mellitus type 2 and hypertension presented with altered mental status, worsening headaches, fevers, photophobia, and neck stiffness. Magnetic resonance imaging (MRI) of the brain demonstrated a prior lacunar infarct in the left basal ganglia. The patient underwent a fluoroscopic guided lumbar puncture (LP). Cerebrospinal fluid (CSF) showed WBC of 400/mm, with lymphocytic predominance, glucose of 41 mg/dL (concomitant serum glucose of 304 mg/dL), protein of 101 mg/dL, and Coccidioides serology of positive immunodiffusion IgG and complement fixation of 1:4. Serum Coccidioides serology demonstrated positive immunodiffusion IgG, immunodiffusion IgM, and complement fixation of 1:256. The patient was diagnosed with disseminated Coccidioidal meningoencephalitis and was discharged on oral Fluconazole 1000 mg daily.
Approximately a month later, the patient presented with worsening mentation; neuroimaging revealed patchy meningitis of the basal cisterns and an acute lacunar infarct of the left caudate nucleus extending into the lentiform nuclei. Incidentally, head and neck computed tomography angiography (CTA) demonstrated a heterogeneous thyroid gland with a hypodense nodule in the left thyroid lobe.
Ultrasound showed avascular exophytic solid nodule measuring 1.7 × 0.95 × 1.1 cm3 in the left thyroid lobe (Figure 1). In addition, there was another ill-defined isoechoic 1.3 × 0.8 × 1.1 cm3 mass with internal calcifications in the left side of the isthmus (Figure 2).

Exophytic solid nodule measuring 1.7 × 0.95 × 1.1 cm3 in left thyroid lobe.
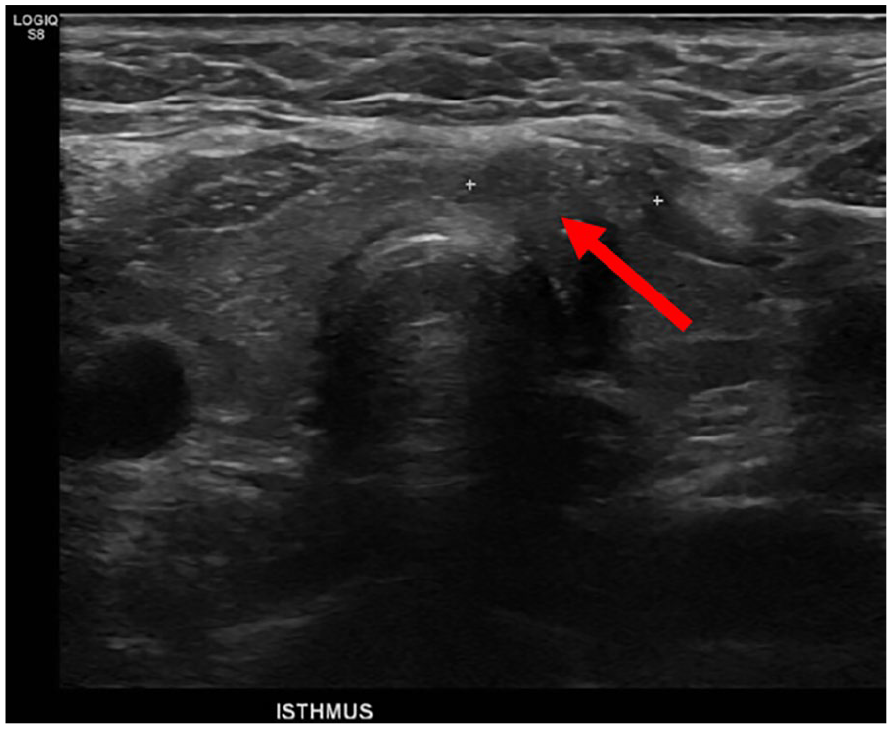
Thyroid ultrasound showing isoechoic 1.3 × 0.8 × 1.1 cm3 nodule with internal calcifications in the left side of the isthmus.
Simultaneously, during this admission, her work up revealed multiple increased foci of uptake, including left thyroid lobe, cervical spine, lumbosacral spine, and left ankle with differential diagnosis of disseminated coccidioidomycosis versus malignancy with metastasis (Figure 3).

Technetium 99 MDP (methyl diphosphonate), whole body bone scan, showing multiple foci of uptake: Left thyroid lobe, cervical spine, lumbosacral spine, and right ankle.
Due to concern for a neoplasm, ultrasound guided Fine Needle Aspiration (FNA) of thyroid nodules were performed. Both sites’ biopsies were consistent with benign follicular nodules without evidence of malignancies. Left lobe nodule, however, revealed presence of Coccidioides spherules with endosporulation (Figures 4 and 5). Serum thyroid-stimulating hormone (TSH) is 0.753 mcIntlUnit/mL (microliter international unit/milliliter), and free thyroxine (T4) is 1.2 ng/dL (nanogram/deciliter), which were within normal limits.
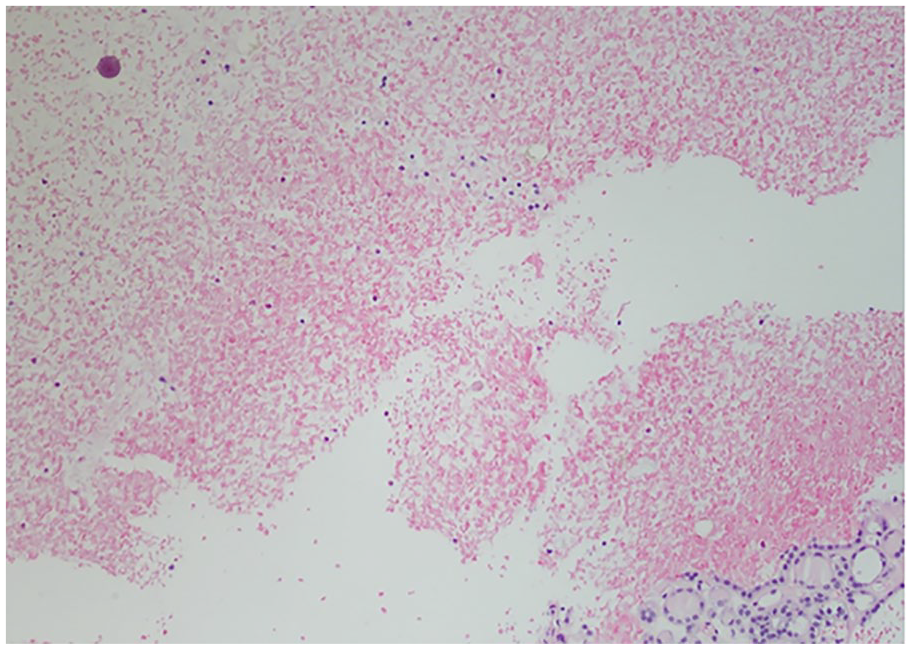
Hematoxylin and eosin stain with 10× magnification showing Coccidioides Spherule.

Hematoxylin and eosin stain with 400× magnification showing Coccidioides Spherule.
She was started on Liposomal Amphotericin B infusions for 12 weeks in addition to oral fluconazole 1000 mg daily. Subsequently, due to development of facial skin hyperpigmentation associated with fluconazole, her treatment was changed to Isavuconazonium 375 mg to be continued lifelong. The drug of choice was Isavuconazonium and not other azoles as itraconazole was avoided due to its negative inotropic effect in patients above 50 years of age. Similarly, Posaconazole is associated with hypertension. It is growing evidence to use Isavuconazonium as the most effective and least toxic azole in treatment of disseminated coccidiomycosis refractory to other azoles.
Discussion
Coccidioidomycosis is an infection caused by inhalation of arthroconidia of Coccidioides. Forty percent of patients develop influenza-like, or pneumonia and rest remain asymptomatic. In only 1 to 5% of cases it disseminates to almost any organ system.1,2 Recognized risk factors for the extrapulmonary disease include extremes of age, African or Filipino ancestry, pregnancy, and immunosuppression. 2
It is a well-established fact of thyroid gland to be resistant to infections due to rich lymphatic and vascular supply, well-developed capsule, and high iodine content. 3
Thyroid gland fungal infections are unusual with aspergillus being most common and second being candida. 4 Most fungal thyroid gland infections are asymptomatic and occur in disseminated form of the disease without clinical impact on thyroid function. 5 Dissemination of coccidiomycosis to thyroid is not an exception and it is rarely reported.
Subacute thyroiditis is reported in few cases.4,5 Autoimmune thyrotoxicosis is reported in a case. 6 Asymptomatic involvement was reported once in a patient with Systemic Lupus Erythematous. 7 It is possible that thyroid involvement has been under-reported. In one necropsy study of disseminated coccidiomycosis by Huntington et al, out of 130 cases, thyroid involvement was found in 9 patients without clinical thyroid dysfunction. 8
Thyroid nodules are common in general population, with a reported prevalence of up to 68% in adults on high-resolution ultrasound. 9 In contrast, this case had 2 suspicious thyroid nodules in the setting of suspicious metastasis versus disseminated coccidiomycosis, which warranted ultrasound to evaluate ACR TIRADS (American College of Radiology Thyroid Imaging Reporting and Data System). The FNA is required only for suspicious nodule like in our case as both nodules were TIRADS 4.
The treatment choice and duration of therapy for disseminated thyroid coccidioidomycosis is only speculative and narrative to the expert opinion due to lack of randomized clinical trials. The nearest equivalent would be the “soft tissue dissemination” at the latest Infectious Diseases Society of America (IDSA) clinical practice guideline. 10 At Valley Fever Institute, we recommend high-dose daily fluconazole (600-800 mg daily based on tolerance) for up to 36 months of therapy. 11 In this case, higher dose of fluconazole (1000 mg) was initially used due to concomitant dissemination to central nervous system. Later, her treatment was changed to Isavuconazonium after she developed cutaneous toxicity with fluconazole. Other azoles such as itraconazole and Posaconazole also could be utilized if no contraindication limiting it use is present as in our case.
Conclusions
We present a rare case of disseminated Coccidioidomycosis of the thyroid. This case demonstrates the importance of considering fungal infections in the differential diagnosis of focal thyroid nodules or gland inflammation, especially when exposed to the area’s endemic to certain fungal infections. FNA of the thyroid is an effective diagnostic tool to establish the diagnosis. Optimal treatment is uncertain but, as per experts’ opinion, can be modeled after disseminated coccidioidomycosis to other soft tissue organs which will be 3 years of oral azoles.
Footnotes
Acknowledgements
Acknowledgments are due to Dr. Arnold Vera (Endocrinologist at UCLA-Harbor Medical Center).
Author’s Note
This article was presented as a poster presentation at the 2019 Western Medical Research Conference on January 23, 2019, at Carmel, California, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics approval to report this case was obtained from Kern Medical Center IRB # 18048.
Informed Consent
Written consent was obtained from the patient for their anonymized information to be published in this article.