
Abstract
Clival osteomyelitis is a potentially life-threatening skull base infection. It is rare and generally challenging to diagnose and treat. Clival osteomyelitis is typically seen in the pediatric population and is very rare in the adult population. It occurs as a complication of recurring paranasal infections and malignant otitis externa. The exact pathophysiology of osteomyelitis of the clivus is relatively uncertain. Here, we describe a case of a 36-year-old man with medical history significant for hypertension and poorly controlled type 1 diabetes mellitus who experienced recurrent paranasal sinus infection for 2 years. He received multiple antibiotic treatments and underwent adenoidectomy without substantial improvement of symptoms. Ultimately, a diagnosis of the clival osteomyelitis through the help of a computed tomography (CT) scan of the paranasal sinus and neck was made. This diagnosis allowed for adequate intervention and treatment of our patient with subsequent resolution of his presenting symptoms. This case highlights the importance of high suspicion for clival osteomyelitis in patients with recurring sinus infections.
Introduction
Clival osteomyelitis is a rare skull base infection usually caused by poor treatment of malignant otitis externa, and in some cases paranasal sinus infection. It is associated with high mortality and morbidity rates especially if left untreated. It is more common in children but can be seen rarely in adults. This case highlights a rare occurrence of clival osteomyelitis in a 36-year-old man with a history of recurrent paranasal infections.
Case Presentation
Our patient is a 36-year-old man with medical history significant for hypertension, type 1 diabetes mellitus, sinusitis, history of tonsillectomy and adenoidectomy (aged 15), and repeat adenoidectomy at the age of 34 with a 2-year history of recurrent ear infections/sinusitis. He presented to the emergency department (ED) with continued symptoms of recurrent ear infections and sinusitis despite multiple courses of antibiotics.

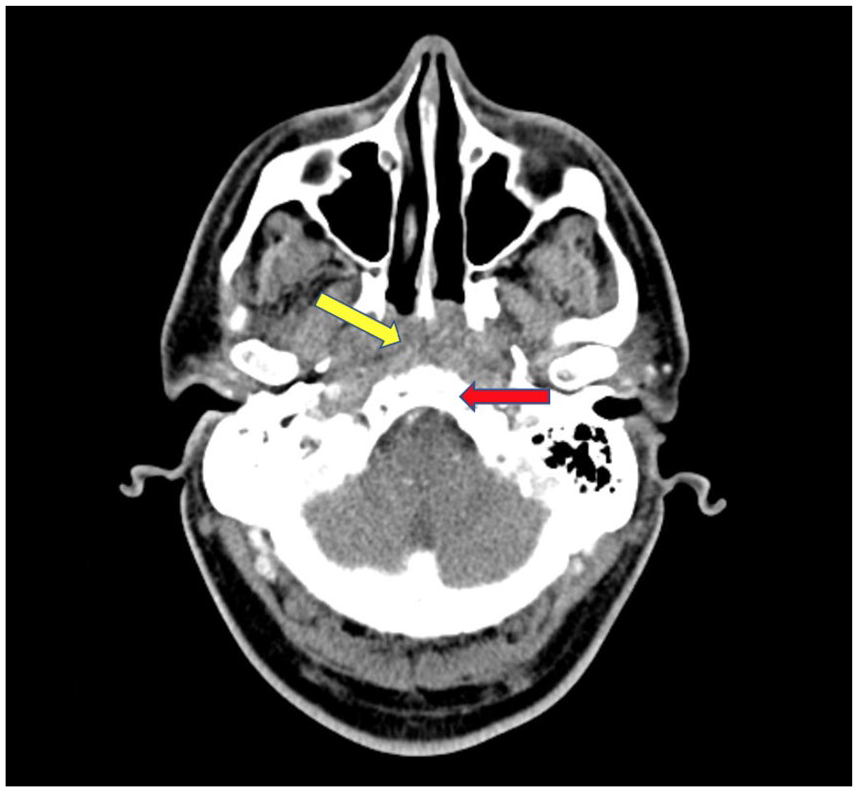
CT head and neck on admission—pharynx: A 1.3 cm × 1.3 cm × 2.8 cm (AP × transverse × CC) fluid collection with foci of air at prevertebral retropharyngeal space (yellow) with adjacent periosteal reaction and bony destruction of the clivus (red). Unremarkable oropharynx and hypopharynx.

CT head on admission—fluid collection with foci of air at prevertebral retropharyngeal space (yellow) with adjacent periosteal reaction and bony destruction of the clivus (red).

CT head and neck showing resolution—there has been progressive resolution of the previously noted osteomyelitis and retropharyngeal abscess with only a small focal area of lucency remaining within the nasopharyngeal soft tissues as noted above.
CT head showing resolution—there has been progressive resolution of the previously noted osteomyelitis and retropharyngeal abscess with only a small focal area of lucency remaining within the nasopharyngeal soft tissues as noted above.
The patient stated that after his second adenoidectomy he began experiencing ear and facial pain. He was subsequently diagnosed with sinusitis and started on amoxicillin. His symptoms failed to resolve, and he later underwent fiberoptic endoscopy by his otolaryngologist, who reported what appeared to be adenoids growing back with some associated purulent drainage. Culture of this drainage grew Klebsiella pneumoniae, and the antibiotic was changed to ciprofloxacin. The patient also endorsed that he was started on trimethoprim/sulfamethoxazole as well. In total, the patient completed three 2-week courses of 3 different antibiotics.
The day prior to presenting to the ED, he had noticed purulent material escaping from his right ear as well as purulent material whenever he blew his nose. He also reported decreased hearing and feeling of fullness in the right ear with associated poor appetite, night sweats, and a weight loss of about 10 pounds in the past several weeks. He denied dizziness, tinnitus, falls, facial tenderness, fevers, or chills at that time. He visited his otolaryngologist physician who performed a right myringotomy and promptly instructed the patient to visit the local ED for further evaluation.
In the ED, he was noted to be afebrile, with heart rate 137 beats per minute, respiration rate (RR) 14, blood pressure (BP) 120/78 mm Hg, saturating 97% on room air. His laboratory tests were significant for glucose 386 (74-118 mg/dL), sodium 128 (136-44 mmol/L), potassium 5.2 (3.6-5.1 mmol/L), HbA1c 14.0 (4.0%-6.2%), white blood cell (WBC) count 15.1 (4.8-10.8 K/µL), polys 72.6 (42%-75%), Lactic acid Point of Care Testing 1.64 (0.5-2.2 mmol/L), acetone negative, and HIV non-reactive. Computed tomography (CT) scan of the paranasal sinuses (see Images 1 and 2) revealed a soft tissue collection within the nasopharynx with areas of destruction of the clivus with maxillary sinus mucosal thickening. Computed tomography of the neck (see Images 1 and 2) showed a 1.3 cm × 1.3 cm × 2.8 cm (anteroposterior × transverse × craniocaudal planes) fluid collection with foci of air at prevertebral retropharyngeal space with adjacent periosteal reaction and bony destruction of the clivus concerning for retropharyngeal abscess with osteomyelitis of the clivus.
Blood and purulent drainage were cultured in the ED, and he was taken to the operating room for incision and drainage. The cultured specimens were sent for fungal and wound cultures. Since he had previously completed multiple courses of antibiotics, there was a concern for the growth of methicillin-resistant Staphylococcus aureus (MRSA) and gram-negative rods, including Pseudomonas. With the patient’s poorly controlled diabetes, there was also a remote possibility of a fungal infection such as aspergillosis or less likely mucormycosis. Due to the reasons previously mentioned, the patient was started on vancomycin and meropenem.
He remained afebrile during this hospitalization with improving leukocytosis. Cultures from the sinus drainage and from the operating room grew Streptococcus group F. After review of culture sensitivities, vancomycin was discontinued while he was continued on meropenem. A right-sided peripherally inserted central catheter line was placed as he required at least 6 weeks of IV antibiotics treatment. The final culture results showed presence of Streptococcus gordonii, a viridans strep. The patient completed 3 weeks of IV antibiotics during hospitalization. Upon discharge, meropenem was discontinued and the patient was started on IV ceftriaxone 2 g daily for 3 weeks plus metronidazole 500 mg p.o. every 8 hours to complete a 6-week course of antibiotics. This regimen was picked to cover S gordonii along with any anaerobic organisms that might have been present. He was further instructed to follow up with Infectious Disease as outpatient and later repeat CT imaging of the face and neck to monitor resolution of the abscess and osteomyelitis. Repeat CT imaging (see Images 3 and 4) after 6 weeks of antibiotic treatment showed progressive resolution of clival osteomyelitis and retropharyngeal abscess. This diagnosis allowed for adequate intervention and treatment of our patient with subsequent resolution of his presenting symptoms.
Discussion
Infection of the clivus bone is a form of skull base osteomyelitis (SBO). Skull base osteomyelitis is rare and challenging to diagnose and treat. Skull base osteomyelitis intends to have high mortality and morbidity rate if not intervened rapidly. 1 The more typical locations of SBO are the temporal and sphenoid bone. In contrast, infection of clivus bone is considered atypical and rarer. 2 This variant can be either idiopathic 3 or spread directly from the paranasal sinus or other adjacent bones of the skull base. 4 The presentation of symptoms of osteomyelitis of the clivus is typically nonspecific. Some of the more common ones include headaches and cranial nerve palsies. In addition, patients tend to have immunocompromised states, including diabetes. 5
The exact pathophysiology of SBO is still relatively uncertain. Most cases have been reported in immunocompromised patients or patients with diabetes. Within this patient population, impaired phagocytosis, poor leukocyte activity, and impaired intracellular breakdown of bacteria are thought to contribute toward osteomyelitis. Furthermore, the cerumen in the ears of patients with diabetes has a higher pH, which contributes to a reduction in the bactericidal properties of cerumen. 6 It is also believed that in some cases, SBO can result secondary to a spreading malignant otitis externa infection. The infection extends from the external ear canal through skull base foramina. Progressive spread can lead to cranial neuropathies as well as possible involvement of the parotid gland as well as the temporomandibular joint. 6
To diagnose SBO, blood tests can be initially conducted. Acute-phase reactants will be consistently elevated, particularly erythrocyte sedimentation rate (ESR). Leukocytosis and an absence of fever are less reliable indicators of SBO. 7 Furthermore, the prominent increase in ESR can be used in 2 ways. First, it can be used to help discriminate between SBO and malignancy. Despite the many similarities in the presentation of these 2 conditions, an elevated ESR would be unusual in a diagnosis of malignancy. 8 Second, it can be used to monitor the response of SBO to treatment. Even more so than laboratory tests, imaging studies can be crucial to diagnosis. The most used diagnostic study is the CT scan, an efficient method to observe the skull. The most significant benefit is that CT scan allows for visualization of bone erosion and demineralization. Magnetic resonance imaging (MRI) can be beneficial as well for visualizing soft tissue components near the skull. It also helps to determine complications such as thrombosis and intracranial spread.
The treatment of SBO firstly entails long-term broad-spectrum antimicrobial agents. However, it is then important to obtain culture results of the offending organism and switch agents to target accordingly. Depending on the offending bacterium, some examples of antibacterial therapy that are typically used include piperacillin-tazobactam, ceftazidime, or ciprofloxacin. 9 Some antifungal regimens used include lipid amphotericin B formulation, posaconazole, voriconazole, itraconazole, and caspofungin. Surgical debridement is often effective for osteomyelitis of fungal origin, while antibiotics work best for bacterial origin. 9 However, surgical treatment is also recommended in cases where an abscess has formed in the joint space of the clivus bone or where extensive bone destruction is observed. 10 Pseudomonas aeruginosa was the most common bacteria cultured, while Aspergillus and Scedosporium were the most common fungus cultured.
Skull base osteomyelitis, in general, has been found to have significant morbidity and mortality. In one study, 48% of the patients suffered lingering cranial nerve abnormalities. Mortality in this patient population was found to be at a rate of 9.5%. 11 Another study found that immunocompromised patients were more susceptible to major complications (P ≤ .001) as well as increased mortality (P ≤ .01). 12 Early diagnosis and treatment are critical in saving lives, especially for those with immunocompromised states, including our patient with long-standing diabetes. Rapid intervention has been demonstrated to lead to more positive outcomes, such as the use of antibiotics in our patient.
Conclusions
This case illustrates a rare case of SBO, in particular clival osteomyelitis, caused by paranasal sinus infection. A high degree of suspicion and early treatment could reduce the morbidity and mortality risk associated with this infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.