
Abstract
Pure red cell aplasia (PRCA) is a rare disorder mainly affecting the erythroid precursor cells. It presents with severe isolated reticulocytopenia with relatively normal counts in the myeloid and megakaryocytic lineages. It has been attributed to numerous congenital and acquired causes. DNA Methyl Transferase 3 Alpha (DNMT3A) mutation has been typically associated with myeloid and lymphoid malignancies. There is a scarcity of data regarding the association of DNMT3A mutation with PRCA. We report a case of a 73-year-old man who initially presented with anemia and reticulocytopenia. After a thorough evaluation and eventual bone marrow biopsy, he was diagnosed with PRCA. Further genetic testing identified a DNMT3A mutation. We are reporting this rare case to highlight the fact that DNMT3A mutation can also present as isolated PRCA in and of itself without the co-occurrence of leukemia, lymphoma, or myelodysplastic syndrome (MDS).
Introduction
Genetic mutations have a significant impact on diagnosis, prognosis, and therapy. Typically, DNA Methyl Transferase 3 Alpha (DNMT3A) mutations are linked with leukemia, lymphoma, or myelodysplastic syndrome (MDS)/myeloproliferative neoplasm (MPN).1-5 It is however important to recognize that this mutation can also occur with pure red cell aplasia (PRCA). Reported data has been lacking for this key association as there are only a few reports with only 4 patients having ever been identified with PRCA and DNMT2A mutation. 6
Case Presentation
A 73-year-old man presented with chest pain while playing golf. His medical history was significant for prostate cancer treated with radical prostatectomy 7 years ago, hypertension, and hyperlipidemia. Initial workup revealed isolated anemia with a hemoglobin of 7.4 g/dL. Myocardial infarction was ruled out and his angina was attributed to cardiac demand ischemia in the setting of anemia. His other blood counts including white blood cells and platelets were normal. Anemia workup revealed normal iron studies but revealed significant reticulocytopenia with a reticulocyte of 0.07% (normal values 0.5%-2.5%).
A thorough and detailed medication history failed to implicate any attributable medications. Nutritional causes of anemia such as iron, vitamin B12, folate, and copper deficiencies were ruled out. Infectious etiologies for common infections such as HIV, hepatitis, and Epstein-Barr virus (EBV) were negative. Parvovirus B-19, which is known to have a strong association with PRCA, was also checked for by polymerase chain reaction (PCR) and was negative. Hemolysis workup was insignificant as lactate dehydrogenase, haptoglobin, and indirect bilirubin were all within normal ranges. Coombs test was also negative. Hemoccult testing negative for any potential gastrointestinal bleeding. Autoimmune workup including an anti-nuclear antibody screen was also unremarkable.
This led us to undergo a bone marrow biopsy. Pathological review showed less than 1% erythroblasts with a mildly hypocellular bone marrow with no signs of dysplasia or neoplastic changes (Picture 1-4). Fluorescent in situ hybridization (FISH) and PCR-gene rearrangement for malignant etiologies were negative. Computerized tomography of the chest was performed to evaluate for any evidence of a thymoma and was negative. Ultimately, an extended cytogenetic testing of the bone marrow revealed DNMT3A mutation.
Discussion
Pure red cell aplasia is a rare disease of the bone marrow characterized by a normochromic normocytic anemia due to maturation arrest of the erythrocytes. 7 Its hallmark feature is severe reticulocytopenia with very low or absent erythroblasts on bone marrow examination. The attributable etiologies include congenital or acquired causes. Acquired PRCA is further subdivided into primary (idiopathic, autoimmune) disorder or secondary disorder.
Some of the congenital conditions that predispose an individual to PRCA include Diamond-Blackfan anemia, Aase syndrome, and Pearson marrow pancreas syndrome.8,9 Primary PRCA is an autoimmune or idiopathic process thought to be mostly caused by an autoantibody-mediated process against the early erythroid precursor cells. 10 Pure red cell aplasia can also be an initial presentation of MDS. 11 Secondary causes of PRCA include drugs, infections, autoimmune disorders, and neoplasms. The most common drugs with an association to PRCA include antibiotics such as trimethoprim-sulfamethoxazole as well as antivirals. Other drugs including antiepileptics, myelosuppressive drugs, as well as immune checkpoint inhibitors have also been attributed to this condition. 12 Viral infections such as Parvovirus B19 have a strong association with PRCA, 13 but other viral infections including EBV, HIV, or viral hepatitis can also act as a trigger. Autoimmune disorders such as systemic lupus erythematosus and rheumatoid arthritis as well as various neoplasms such as chronic lymphocytic leukemia (CLL), chronic myeloid leukemia (CML), non-Hodgkin lymphoma, Hodgkin lymphoma, and multiple myeloma have all been associated with PRCA. Patients with PRCA can also be found to have a thymoma in up to 20% of cases, thus all patients found to have PRCA should be investigated with imaging of the chest. 14
Initial laboratory evaluation consists of a thorough workup for causes of anemia. Reticulocytopenia is a key feature with reticulocytes often below 10 000/µL. Microscopic evaluation of a blood smear most often shows a normocytic normochromic anemia with no significant spherocytes or fragmented red cells. Hemolytic markers including lactate dehydrogenase, haptoglobin, indirect bilirubin, and direct antiglobulin test are all typically normal as hemolysis is not usually associated with PRCA. All patients suspected of PRCA require a bone marrow confirmation. The diagnostic criteria consists of (1) reticulocytopenia <10 000/µL; (2) normocytic, normochromic anemia; (3) normocellular bone marrow with erythroblasts <1%; (4) normal white blood cell (WBC) and platelet counts; and (5) absence of other abnormalities in the myeloid cells, lymphocytes, or megakaryocytes (CLL or CML may however co-occur in certain situations). 15
Treatment of PRCA depends on the severity at presentation and the underlying etiologies implicated. Oftentimes, PRCA can result in spontaneous remission. Initial observation of patients for weeks to months with close laboratory monitoring of the hemoglobin may not be unreasonable. Treatment of any potential underlying causes also remains an integral part of management. Therapeutic agents employed are mainly immunosuppressive or immunomodulatory medications, although there are no high-quality data regarding their efficacy. Glucocorticoids such as prednisone are often initially employed with an extended taper dosing and subsequently transitioned to immunosuppressive agents such as cyclosporine. 7 Refractory cases are treated with cyclophosphamide, azathioprine, rituximab, or sirolimus. Allogenic transplant can also be considered if patients remain refractory. 16
DNMT3A is a gene that encodes DNA methyltransferase enzyme which regulates DNA methylation. This is essential for epigenetic modifications, transcriptional regulation, and gene expression. Mutations of DNMT3A have been detected in primary MDS patients, some of which progress to acute myeloid leukemia. 17 DNMT3A mutation is also observed in MPN, CML, T cell leukemia, lymphoma, and mixed phenotypic acute leukemia. 18 Based on our literature review, there is paucity of data which links DNMT3A mutation to isolated PRCA. We have cited the only other report which describes 4 patients who were observed to have this correlation. 6
We acknowledge that acquired PRCA can be an initial presentation of MDS. However, we have had no evidence of MDS on our pathological specimens nor do we have any other cytopenias or blasts on laboratory indices to suspect this. He is being maintained on cyclosporine with hemoglobin parameters consistently >11 g/dL. He is also actively being monitored for any laboratorial or clinical changes that may warrant further investigation. Given our findings as well as previously reported data, DNMT3A mutation should be recognized as a possible mutation in patients with PRCA. Further investigations are warranted to validate our findings.

Hematoxylin and eosin (H&E) stain showing normocellular bone marrow of core biopsy.

H&E stain: granulocytic lineage, megakaryocytes, and lymphocytes. Absence of erythroid precursors.

Myeloperoxidase (MPO) staining showing granulocytic lineage.
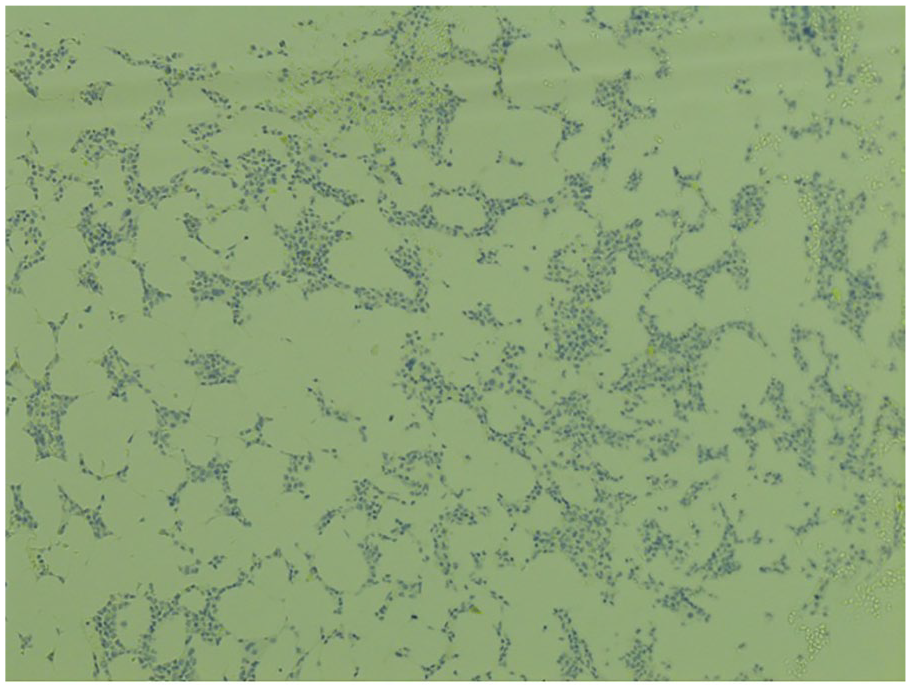
Epithelial cadherin showing essentially absence of erythroid precursors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.