
Abstract
Risk factors for infective endocarditis (IE) include congenital heart defects, poor dentition, immunosuppression, or recent instrumentation. The occupational hazard of a dog bite, combined with bicuspid aortic valve (BAV) led to IE. 16S ribosomal DNA was able to pinpoint the causative organism. A healthy 33-year-old postman presented in profound heart failure and sepsis due to aortic regurgitation and an aortic root abscess. He underwent emergency aortic valve replacement and was found to have a BAV and anomalous right coronary artery. Blood cultures remained negative. 16S ribosomal DNA polymerase chain reaction (PCR) revealed the causative organism was Capnocytophaga canimorsus. On review, he recalled receiving a dog bite followed by a febrile illness a few days later. Congenital BAVs may become infected by seemingly innocuous injuries. 16S rDNA PCR is a more sensitive and specific diagnostic test than culture. This case demonstrates its utility in providing appropriate antimicrobial management for IE.
Highlights
Congenital bicuspid aortic valves may become infected by seemingly innocuous injuries. 16S rDNA polymerase chain reaction (PCR) from tissue samples is a more sensitive and specific diagnostic test than culture. This textbook case demonstrates the utility of 16S rDNA PCR in providing appropriate antimicrobial management for infective endocarditis.
Background
Acute heart failure (HF) from aortic regurgitation and infective endocarditis (IE), with root abscess, is an emergency. Without treatment, IE is uniformly fatal. Complex scenarios involving IE require a dedicated heart team, consisting of cardiothoracic surgeons, clinical microbiologists, and cardiologists. Guidelines from the European Association of Cardiothoracic Surgery (EACTS) and European Society of Cardiology (ESC) recommend urgent surgery for IE associated with aortic regurgitation, left ventricular dilatation, and HF.
Case Report
A healthy 33-year-old postman developed night sweats and shortness of breath. Numerous general practitioner (GP) tele-consultations prompted severe acute respiratory syndrome corona virus 2 (SARS-CoV2) testing. He received 3 courses of oral antimicrobials for presumed lower respiratory tract infection with negative PCR for SARS-CoV2.
Three months later, progressive dyspnoea resulted in an emergency admission to hospital, with acute decompensated HF, requiring inotropic support. Computed tomography pulmonary angiogram ruled out pulmonary embolism and revealed profound pulmonary oedema. Echocardiogram demonstrated severe aortic regurgitation, with vegetations on the noncoronary cusp and an aortic root abscess (Figure 1).

Transoesophageal echocardiogram image demonstrating large vegetation on noncoronary cusp.
He underwent urgent early aortic valve replacement with a 25 mm carbomedics mechanical aortic valve as per International Guidelines (Class 1 Indication). 1 Intraoperatively, he was noted to have a congenital abnormality: a bicuspid aortic valve (BAV), with fusion of right and left coronary cusps, and anomalous origin of his right coronary artery from his left main stem.
The patient was empirically commenced on an antibiotic regimen for IE; ceftriaxone, vancomycin, and gentamicin. Five sets of blood cultures failed to yield an organism after prolonged incubation. Valve tissue culture yielded no growth. The history of his illness and potential cause of endocarditis was reviewed multiple times. He had no recent dental treatment, change in bowel habit or history of recent instrumentation. On reading a pamphlet about IE, he recalled a dog bite on his index finger, whilst delivering a letter. Three days later, he developed night sweats and rigors which prompted his first GP consultation for testing of SARS CoV2.
C. canimorsus was revealed as the causative pathogen following 16S rDNA sequencing of the valve tissue undertaken by Public Health, England. Gentamicin and vancomycin were stopped after 14 days of treatment. Targeted treatment with ceftriaxone 2 g OD was continued for a total of 6 weeks treatment. He had an uneventful postoperative course and was discharged when he changed to oral antibiotics and was stable on warfarin, on the 14th postoperative day.
Discussion
Congenital Abnormality
Congenital coronary artery anomalies are estimated to occur in 0.3% to 1.3% of the population. 2 Most cases are asymptomatic incidental findings; however, certain anomalies increase the risk of myocardial ischemia, HF, or sudden cardiac death. Angelini, in particular, found left anomalous coronary artery from the opposite sinus of Valsalva (ACAOS) posed such a risk that surgical revascularisation is warranted.3,4 However, whether surgery is indicated for right ACAOS is less clear. 4 There was no statistically significant survival benefit in surgical management versus medical management among 247 patients with anomalous coronary arteries who were followed for 10 years, in what the authors perceived as an asymptomatic variant. 5 Intramural aortic courses (IACs) of anomalous coronary arteries may also increase the risk of developing ischemia in the setting of compression from an aortic valve replacement. In systole, the aorta stretching may predispose patients to constriction of an intramural anomalous coronary artery. The intercoronary commissure may compress the anomalous vessel in diastole also. Anomalous coronary arteries may also be atretic as a consequence of developmental haemodynamics. 5 The slit-like orifice, and acute angle of take-off, creates a haemodynamic effect similar to an ostial stenosis, which reduces coronary blood flow. 5 This is why deroofing may be advocated for over bypass grafting. In Guidelines for the Management of Adults With Congenital Heart Disease, anomalous left coronary artery from the right (ALCA-R) with IAC should be revascularized. (Class- I recommendation). 6 In anomalous right coronary artery from the left sinus (ARCA-L), revascularization is only advocated for in the presence of documented ischemia, sudden death, or unexplained arrhythmia (Class-I recommendation), but multidisciplinary team management could support the decision for surgical repair in asymptomatic cases (Class-IIa recommendation). 5 In our case, we elected not to bypass the right ACAOS as the patient was asymptomatic and the prognostic benefit of bypass in his case, was questionable.
The BAV was found to have fusion of right and left coronary cusps, Sievers Type 1. Abnormal valvulogenesis results in BAV. Adjacent cusps fail to split, leaving only 2 cusps, 1 of which is frequently larger than the other. The morphology of the commissures changes depending on how they are united. In roughly 2% of individuals with a BAV, anomalies in coronary artery anatomy, such as anomalous origins of coronary arteries and upwardly displaced coronary ostia, are found. 7 The autosomal-dominant inheritance pattern for BAV is regarded to be the most prevalent, but there is evidence of genetic variability, and the pattern may be varied. 7 It is a Class-1 recommendation from the American College of Cardiology and the American Heart Association to screen relatives using echocardiography in first degree relatives.6 -9 This man’s family have been referred for screening.
Capnocytophaga Canimorsus
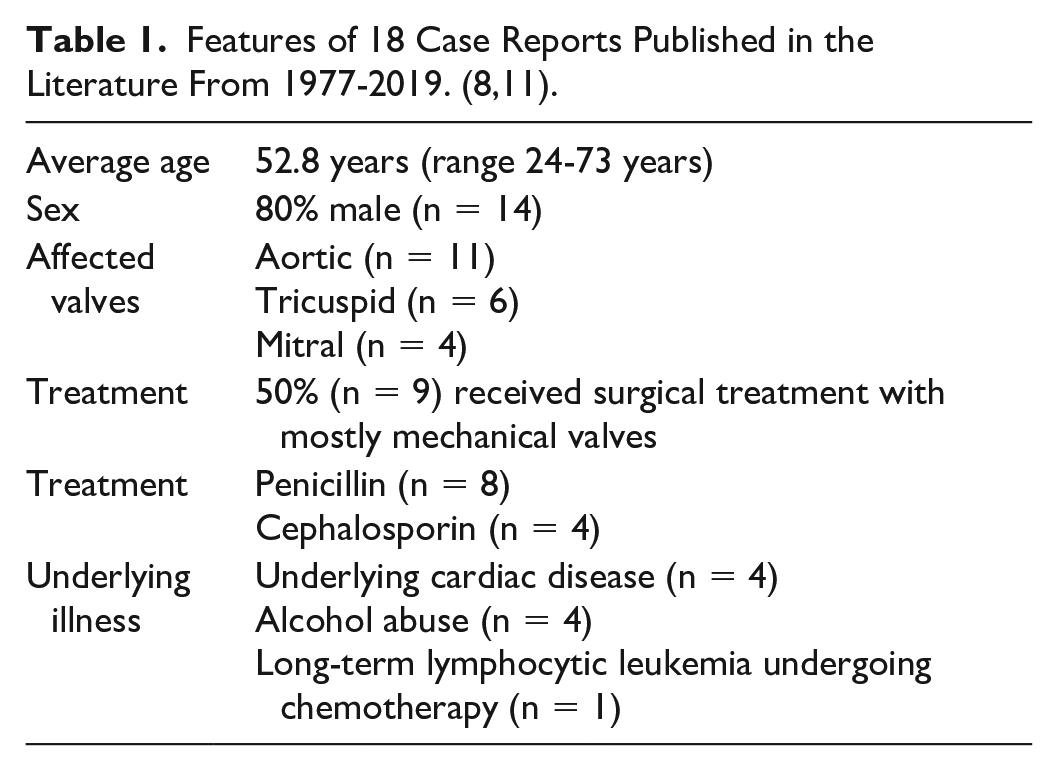
C. canimorsus is a facultatively anaerobic, fastidious Gram-negative bacillus considered to be a commensal oral flora in dogs. It was originally described by Bobo & Newton in 1976 in a patient with meningitis. Patients who are immunocompromised, particularly with asplenia and alcoholics are predisposed to severe infections with fulminant sepsis. It has been associated with a wide variety of infections including meningitis, septic arthritis, and IE. 8 Infective endocarditis accounts for under 2% of C. canimorsus blood stream infections and is rare. Between 1977 and 2019, there were 18 cases of C. canimorsus IE reported in the literature (Table 1). Twelve of these cases had animal contact with a dog, 1 with a lion, and in 5 cases animal contact was not described. 10 Recent publications report B-lactamse production in between 32% and 70% of isolates. A Class-D beta-lactamase has been described among in 4 strains of C. canimorsus. This gene, designated ‘blaOXA-347, is phenotypically associated with resistance to penicillin, cephalosporins, and imipenem and is classified as a carbapenemase.
Features of 18 Case Reports Published in the Literature From 1977-2019. (8,11).
Bacterial Identification
Historically, phenotypic identification of bacteria was only available, but with the advent of proteomics, it has been possible to identify phylogenetically related species within geni. Molecular methods such as full gene sequencing, genomic restriction analysis, conventional ribotyping, 16S-23S intergenic spacer gene sequencing may be utilized for intrageneric differentiation of bacterial species. 11 Bacterial 16S rRNA gene sequencing is commonly used for bacterial identification of culture-negative samples. All bacteria have the 16S rRNA gene, which is an exceptionally maintained segment in the 30 S subunit, the transcriptional engine. 11 Ubiquitous PCR primers may be constructed to select the conserved sections of the 16S gene, allowing for the amplification of the gene in a variety of microorganisms from a lone specimen. The 16S rRNA gene has both conserved and varied sections, which allows for global amplification and discrimination amongst bacteria. For most bacteria and archaea, public databases provide type strains of 16S rRNA gene sequences. In this case, 16SPCR of the infected valve tissue clenched the diagnosis and provided justification for targeted antimicrobial treatment. The patient would otherwise have been treated with a broader regimen increasing the risk of adverse drug reactions and increased healthcare cost.
In conclusion, this textbook case demonstrates the risk factors for IE, the complex multidisciplinary decision-making surrounding management for IE and the utility of 16S PCR in providing appropriate antimicrobial management.
Footnotes
Author’s Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for publication of this report and any accompanying images. A copy of the written consent is available for review from the Editor-in-Chief of this journal.