
Abstract
Primary biliary cholangitis (PBC) is a rare autoimmune disease characterized by intralobular bile duct destruction. Patients typically present with generalized symptoms including fatigue and pruritis, and less commonly, manifestations of lipid deposition including xanthomas and xanthelasmas. We report a case of a 31-year-old female with PBC-associated cirrhosis who had cutaneous xanthelasmas and diffuse gastric xanthomas secondary to hyperlipidemia and lipoprotein X that completely resolved following liver transplantation. While gastric xanthomas have been reported in patients with PBC previously, to our knowledge, this is the first case report of diffuse gastric xanthomas secondary to PBC reported to resolve following liver transplantation, suggesting that liver transplantation is curative for gastric xanthomatosis in patients with PBC-related cirrhosis.
Keywords
Introduction
Primary biliary cholangitis (PBC) is characterized by progressive immune-mediated destruction of intralobular bile ducts leading to cholestasis and eventually fibrosis. 1 It typically presents in middle-aged females with fatigue and pruritis. On physical exam, hyperpigmentation is common while xanthelasmas and xanthomas are present in less than 10% of patients. 2 Laboratory testing most often reveals a cholestatic pattern of liver injury, with particularly elevated alkaline phosphatase and positive antimitochondrial antibody (AMA) testing. AMA is positive in 95% of patients with PBC and is sufficient for diagnosis when found in conjunction with elevated alkaline phosphatase although liver biopsy can be performed as well. Hyperlipidemia is found in most patients although is not associated with increased atherosclerotic risk. 3 We present a patient with profound dermatologic and gastric manifestations of hyperlipidemia secondary to PBC and lipoprotein X (Lp-X) who experienced complete resolution following liver transplantation.
Case Presentation
A previously healthy 31-year-old female presented with a 1-month history of jaundice. She had recently undergone cholecystectomy without improvement. In addition to jaundice and extreme fatigue, she endorsed xerostomia and unintentional weight loss secondary to early satiety. Physical exam revealed scleral icterus, hepatomegaly, and xanthelasmas, most striking on the hands (Figure 1) and around the eyes. Laboratory evaluation was significant for total bilirubin 7.8 mg/dL, aspartate aminotransferase 80 units/L, alanine aminotransferase 57 units/L, and alkaline phosphatase 1028 units/L. Total cholesterol was 1168 mg/dL and low-density lipoprotein (LDL) was measured as greater than 1200 mg/dL. Subsequent lipoprotein metabolism assay revealed the presence of Lp-X, which was mistakenly identified as LDL on initial testing. The serum AMA was positive (1:320) and florid duct lesions and nodule formation on liver biopsy confirmed a diagnosis of primary biliary cholangitis and cirrhosis.

Xanthelasmas on hands of patient at initial presentation.
An esophagogastroduodenoscopy (performed for variceal screening) revealed xanthomas coating the gastric mucosa (Figures 2 and 3), which were confirmed by hematoxylin and eosin (H&E) staining on histopathology (Figure 4). The patient had no response to ursodeoxycholic acid and was subsequently listed for liver transplantation for worsening Model for End-Stage Liver Disease (MELD) score. At 2 months following transplantation, she achieved complete resolution of cutaneous as well as gastric xanthomas, verified with endoscopy.
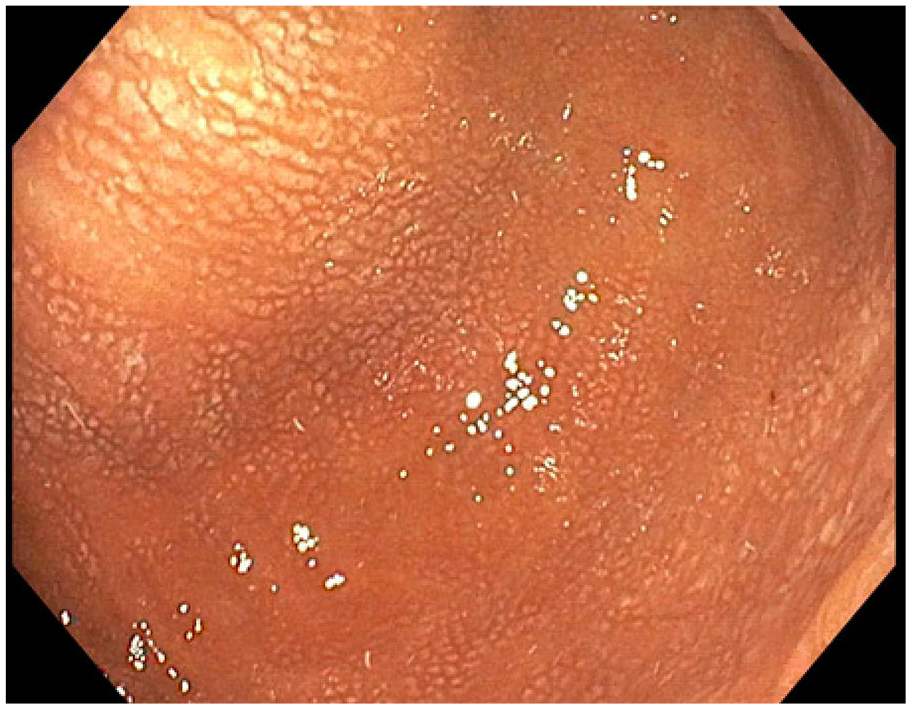
Gastric xanthomas on endoscopy.

Close-up gastric xanthomas on endoscopy.
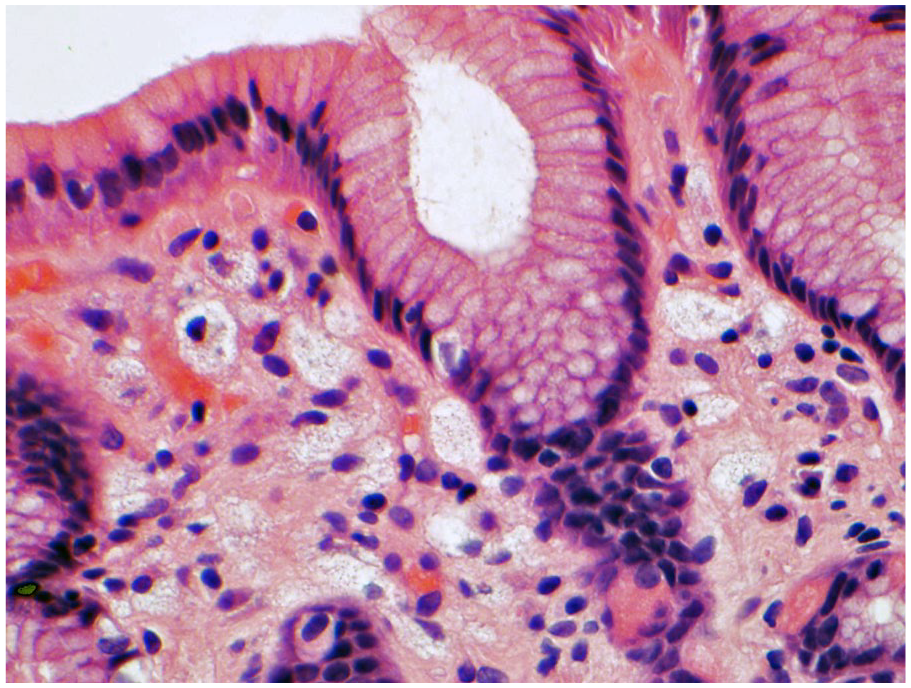
Foamy histiocytes within the lamina propria consistent with xanthoma (hematoxylin and eosin stain).
Discussion
Jaundice and xanthomas are late manifestations of PBC. Xanthelasmas and xanthomas arise secondary to hypercholesterolemia and are typically found surrounding the eyelids and on the palms. Gastric xanthomas are most often singular, and a small number of case reports have described gastric xanthomas in conjunction with Helicobacter pylori infection. Gastric xanthomatosis in a patient later diagnosed with H pylori and PBC has been described. 4
Although hypercholesteremia is present in most patients diagnosed with PBC and responsible for xanthelasmas and xanthomas, it alone does not place patients at higher risk for atherosclerotic events.5,6 Lp-X is often largely responsible for the significant elevations of cholesterol demonstrated in patients with PBC. Lp-X is an abnormal lipoprotein made up of phospholipids and unesterified cholesterol found in the plasma of patients with cholestasis, lecithin-cholesterol-acyl-transferase (LCAT) deficiency or following lipid infusion. 7 It is often erroneously measured as LDL by ultracentrifugation due to similar densities of the molecules.
Lp-X has anti-atherogenic properties by reducing LDL oxidation and preserving endothelial homeostasis. 8 Unlike other lipoproteins, it does not contain Apolipoprotein B100 and lacks micellar structure. 9 High Lp-X levels have been demonstrated in patients with various cholestatic liver diseases, including viral and drug-induced hepatitis and obstructive cholestasis, in addition to PBC. This is suspected to cause plasma hyperviscosity or planar xanthomata, which rapidly improves following resolution of cholestasis. 10 In severe cases, plasmapheresis to rapidly remove Lp-X can be considered, but treating the underlying etiology of cholestasis is recommended as definitive management. 9
Ursodeoxycholic acid is the mainstay of treatment for PBC as it has been shown to lead to both improvement in cholestasis and modification of cholesterol metabolism. 11 Clinical trials have demonstrated it can slow progression of disease and reduce sequelae of cirrhosis.12,13 In patients without decompensated liver disease, obeticholic acid can be used in conjunction with ursodeoxycholic acid or as monotherapy. 14 When patients present late in the disease stage, pharmaceutical therapy is often unsuccessful and liver transplantation is required.
Hyperlipidemia and associated xanthomas and xanthelasmas of the skin are often seen to resolve posttransplantation. To our knowledge, this is the first case report of diffuse gastric xanthomas secondary to PBC reported to resolve after liver transplantation, suggesting that liver transplantation is curative for gastric xanthomatosis in patients with PBC-related cirrhosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Our institution does not require ethical approval for reporting individual cases or case series. Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.