
Abstract
Median arcuate ligament syndrome (MALS), also known as celiac artery compression syndrome, is a rare gastrointestinal condition with an estimated incidence of 2 per 100 000 population. Predominantly in female patients, this syndrome is characterized by the compression of the celiac artery at its origin from the aorta by the median arcuate ligament, which at the same time is entrapping the celiac plexus, causing upper abdominal pain, notably postprandial pain, as well as nausea, vomiting, food aversion, and weight loss. We present a case of abdominal pain secondary to MALS that was appropriately diagnosed after requiring narcotic medication, which responded to surgical therapy.
Introduction
Median arcuate ligament syndrome (MALS), also known as celiac artery compression syndrome, is a rare diagnosis only deduced after excluding more common entities. Compression results from either a low insertion of the diaphragmatic fibers or a high origin of the celiac artery resulting in compression of the celiac ganglion and its associated fibers. 1 However, not all patients with this anatomic compression are symptomatic. The median arcuate ligament is a band of fibrous tissue that passes over the aorta, essentially providing a “tunnel” as the aorta passes through the diaphragm (Figure 1).
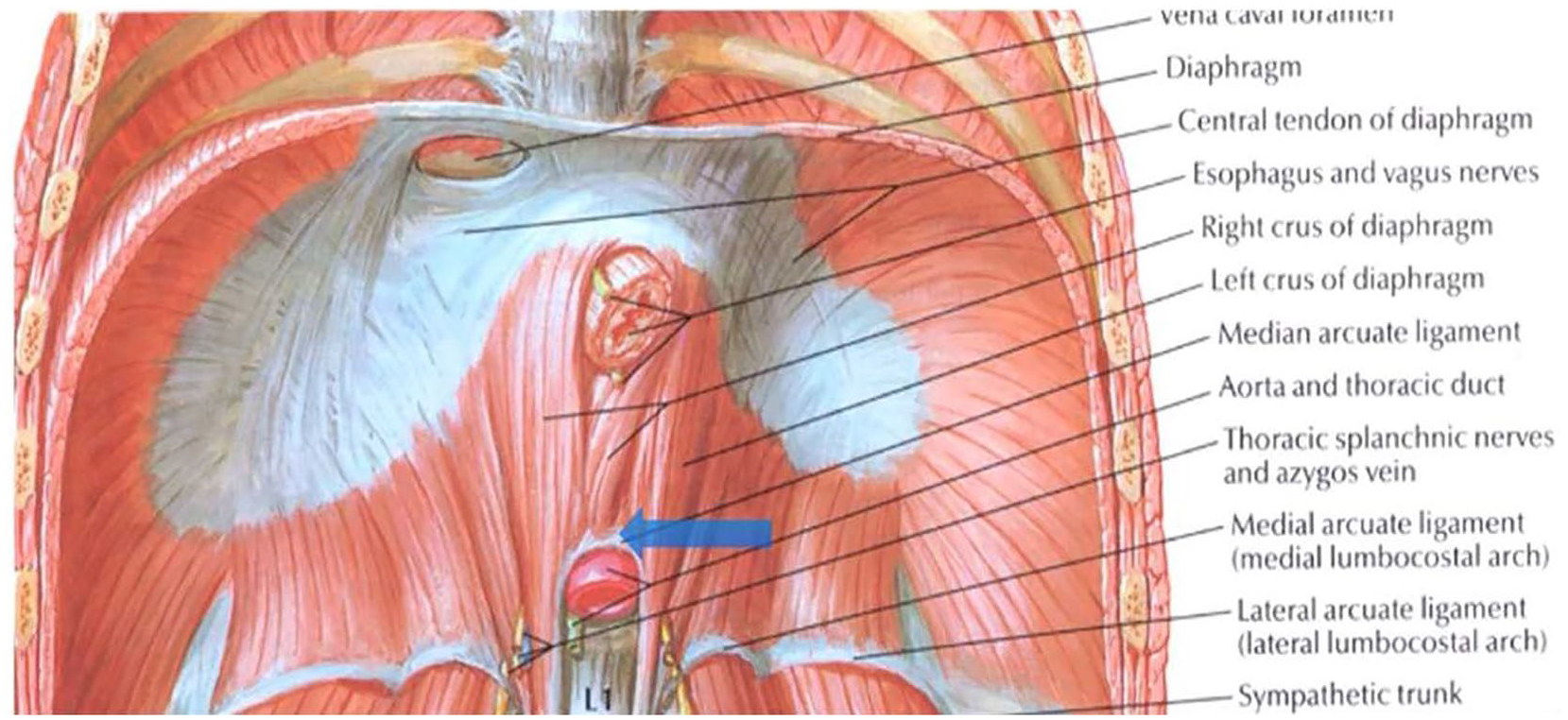
Anatomical association of the median arcuate ligament (MAL) to the diaphragm and aorta. Blue arrow highlights the location of the MAL.
The true prevalence of MALS is uncertain as standardized diagnostic criteria have not been established, and patients can vary in presentation. Typically, females are affected (4:1), and the median age is between 30 and 50 years. 4 Patients present with chronic abdominal pain, which may be worsened with exercise and is generally accompanied by nausea, vomiting, and gastroparesis, resulting in food aversion and weight loss. 5 Al-Bayati et al reported that abdominal bruits could be appreciated on physical examination with abdominal auscultation in approximately 35% of patients. 2
Here, we present a case of intermittent epigastric/left upper quadrant pain not helped with omeprazole and requiring some narcotic use before eventually being diagnosed with MALS.
Case Presentation
A 48-year-old female with a past medical history significant for diabetes mellitus, hypertension, hyperlipidemia, and arthritis presented with an 8-month history of intermittent left upper quadrant pain. The pain was described as sharp, nonradiating, with fluctuating intensity (reported to be 10/10 at worst), not associated with meals, and aggravated by positional changes (laying on her right side and direct palpation). She reported having a 3-year history of intermittent postprandial heartburn with particular foods, which was improved, but not completely relieved, by omeprazole 20 mg twice a day. She also endorsed periodic consumption of narcotic medication to alleviate her pain. She denied fever, chills, weight loss, chest pain, shortness of breath, nausea, vomiting, dysphagia, odynophagia, hematemesis, hematochezia, and melena. Physical examination was pertinent for a soft, nondistended abdomen tender to palpation in the left upper quadrant.
An abdominal computed tomographic (CT) scan was performed, which was interpreted as having no abnormalities. An esophageal motility study indicated a mildly hypertensive lower esophageal sphincter with the smooth muscle portion of the esophageal body, meeting the criteria for diffuse esophageal spasm. Upper endoscopy was significant for a 1 cm hiatal hernia and an erythematous duodenopathy. Colonoscopy was significant for nonbleeding internal and external hemorrhoids but otherwise normal. A nuclear medicine gastric emptying study was attempted. However, the study was prematurely stopped because the patient did not consume the standardized meal of egg and toast because of premature fullness and satiety. A repeat gastric emptying study was recommended. An abdominal ultrasound with a Doppler suggested a spectral waveform of the celiac artery suspicious for MALS. On inspiration, peak systolic velocity was 297 cm/s, and end-diastolic velocity was 112 cm/s (Figure 2). On expiration, the peak systolic velocity was 607 cm/s, and end-diastolic velocity was 185 cm/s (Figure 2). A mesenteric arteriogram was subsequently performed and confirmed the stenosis of the celiac artery, which was accentuated with end-expiration (Figure 3).
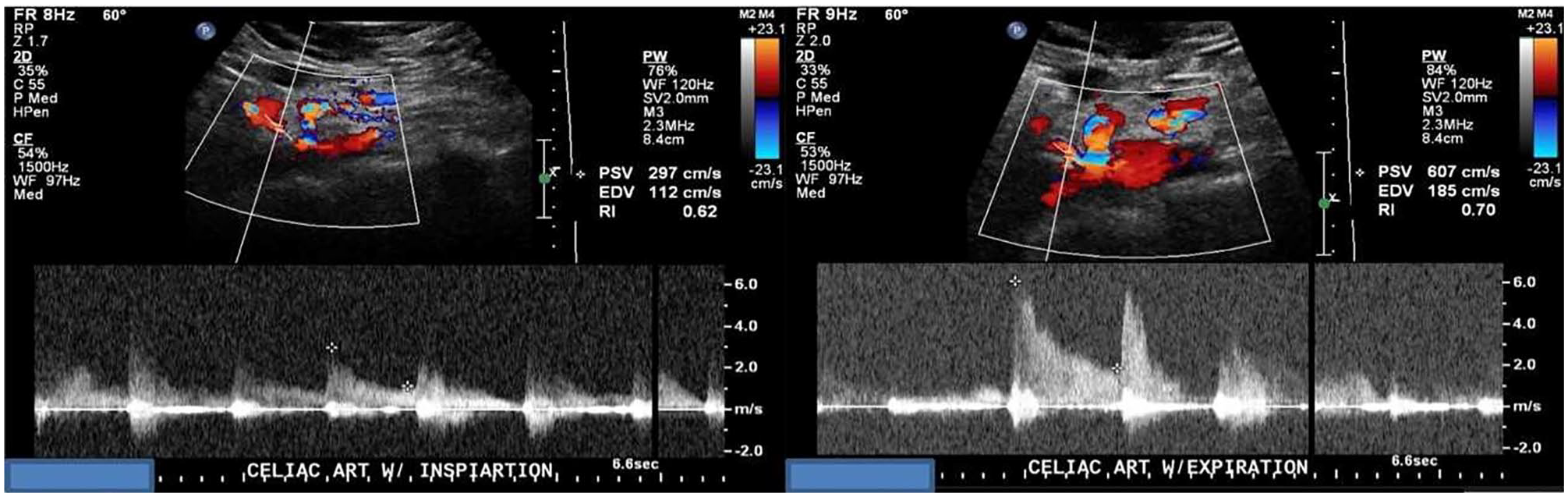
Preoperative duplex ultrasound with inspiration (Left) and expiration (Right).

A mesenteric arteriogram confirming stenosis of the celiac artery (Red Arrow).
The patient underwent a robotic laparotomy with a median arcuate ligament release procedure. Preoperatively, the expiration peak velocity was approximately 600 cm/s, and the inspiration peak velocity was approximately 300 cm/s. Intraoperatively, the patient was found to have an expiration peak velocity of 169 cm/s and an inspiration peak velocity of 109 cm/s (Figure 4). Two weeks after the procedure, the patient reported significant improvement in her abdominal pain compared with before her surgery.

Postoperative duplex ultrasound Doppler with inspiration (Left) and expiration (Right).
Discussion
Median arcuate ligament syndrome is a rare entity seen in approximately 0.002% of the population. 6 Females dominate this condition, comprising up to 83.9% of the total MALS patient population. 7 The etiology of this syndrome is interestingly not due to the compression of the celiac artery leading to foregut ischemia but because of compression of the celiac ganglion, along with its associated sympathetic pain fibers by the median arcuate ligament.
Before diving into the specifics of this syndrome, it is essential to know when it first fell under the spotlight of medicine. In 1917, Lipshutz was the first to describe what we know as MALS today.7,8 The clinical presentation typically consists of nausea, vomiting, postprandial pain, and weight loss symptoms, which can also be present across a spectrum of more common etiologies of abdominal pain. Epigastric pain has been the most reported symptom in 100% of patients, weight loss in 48% to 67% of patients, and nausea and diarrhea in approximately 8% to 10% of patients.8 -10
The MALS can be detected in a percentage of the population who are asymptomatic. The workup focuses on ruling out the more common etiologies of upper abdominal pain such as peptic ulcer disease, gastritis, intestinal ischemia, inflammatory bowel disease, and gallbladder problems. Diagnosis is typically suspected when visualization is seen on a computerized angiogram and Doppler ultrasound. The MALS can confidently be diagnosed with abdominal duplex ultrasound when celiac artery blood flow velocities reach above 200 cm/s during expiration. 11 Our patient reproduced these findings when the duplex ultrasound was performed. The gold standard for MALS diagnosis remains angiography, as it allows direct visual evidence of the celiac artery and celiac ganglion compression accentuated by expiration.
Therapeutic intervention of MALS primarily consists of open/laparoscopic surgical release of the median arcuate ligament, which essentially results in celiac ganglionectomy. In a systematic review of 504 cases, patients undergoing laparoscopic treatment were found to have shorter hospital time and a shorter operative time than open surgical release. 12 As the abdominal pain and other symptoms are not related to ischemia, balloon angioplasty is not an option. Another approach is the use of endoscopic ultrasound to guide injection of the celiac plexus with steroids and/or lidocaine. This gives a brief period of relief and could be used as a preoperative trial. If this celiac plexus block is effective, Kim et al describe some emerging therapies with MAL treatment, including robotic-assisted MAL division with neurolysis. Although this method requires further study, current studies suggest it is an effective treatment. 13
Most importantly, patients who underwent surgical decompression experienced immediate postoperative relief in an estimated 80% of patients. 9 Coelho et al, assessed the outcome of patients’ status post-laparoscopic treatment of MAL, all were found to be asymptomatic at a 3-month follow-up. 10
Our patient’s presentation was atypical in that her pain was both epigastric and left upper quadrant pain, which made establishing the diagnosis even more clinically challenging. We present this case of MALS to highlight the importance of maintaining a broad differential diagnosis when assessing abdominal pain. One should particularly include MALS as a possible source when the abdominal pain is not responding to a “standard” approach and is beginning to require narcotic medications to gain control of the pain.
Conclusion
The MALS is an uncommon condition that should be considered after excluding other more common etiologies of abdominal pain, one can consider MALS as a potential culprit. Diagnostic modalities rely on CT angiogram, US Doppler with blood flow, and ultimately angiogram as its gold standard. Surgical release provides the most significant relief, and there is an evolving role for endoscopic ultrasound-guided celiac block.
Footnotes
Authors’ Note
This case was presented in the Southern Regional Meeting 2022 meeting in New Orleans as a poster presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.