
Abstract
Acute esophageal necrosis (AEN) is a condition characterized by black appearance and inflammation of the esophagus. Our patient developed AEN presenting in the setting of alcohol intoxication and extensive inferior vena cava thrombosis. Esophagogastroduodenoscopy showed blood and black discoloration of the middle and lower esophagus with oozing. To control bleeding, a self-expandable fully covered metallic esophageal stent was placed. Multiple studies and reviews agree that the initial management for AEN is supportive care, resuscitation, and proton pump inhibitors to protect the esophageal mucosa from injury from acid reflux. Our case highlights the benefits of esophageal stent placement to manage AEN with active bleeding.
Introduction
Acute esophageal necrosis (AEN) is a rare condition characterized by black necrotic appearance of esophageal mucosa. 1 The emergence of new endoscopic interventions such as stenting may provide an important treatment option. There are multiple suggested causes to explain the pathogenesis of black esophagus, including ischemia, infections, gastric outlet obstruction, medications (in particular antipsychotic medications), hypercoagulable state, diabetic ketoacidosis, hypoproteinemia, cirrhosis, malignancy, and caustic injury. 2 While supportive care is the main therapy for this condition, our patient was managed with placement of a fully covered self-expandable stent to control active bleeding and possibly prevent further complications.
Case Report
A 58-year-old man with a history of alcohol abuse was admitted for epigastric pain, chest pain, and dyspnea. The patient had sustained a fall 4 months prior to admission, and since then, had been sedentary, usually staying in bed. He drank 5 glasses of whiskey daily and smoked tobacco, 3 to 4 packs daily for 40 years. Vital signs on admission were unremarkable. He had a white cell count of 15 000/uL, hemoglobin of 13.8 gm/dL, platelets of 154 000/uL, and an INR of 1.2 with normal creatinine. Initial lactic acid was 7 mmol/L. It normalized after fluid resuscitation. Liver tests showed bilirubin 2.6 mg/dL, direct bilirubin 1.6 mg/dL, alkaline phosphatase 161 IU/L, aspartate aminotransferase 275 IU/L, and alanine aminotransferase 78 IU/L. Computed tomography (CT) showed hepatic steatosis and a large inferior vena cava (IVC) thrombus from the level of renal veins extending to the left internal iliac vein. It also showed irregularity in the duodenum and gastric antrum with gastric distension and thickened, fluid-filled esophagus.
He was initially treated with heparin for anticoagulation; however, he developed hematemesis and anticoagulation was held. The patient continued to be hemodynamically stable. His hemoglobin dropped to 11.4 gm/dL, but he did not require blood transfusion. An esophagogastroduodenoscopy (EGD) showed red and dark blood in the lower third of the esophagus, diffuse severe necrosis, and black discoloration in the middle and lower third (Figure 1). There was active bleeding in the middle esophagus. No abnormalities were seen in the stomach and duodenum. To obtain hemostasis, a fully covered, self-expanding 15 cm (Wallflex covered 23 mm by 15 cm) stent was placed in the esophagus, 23 cm distal to the incisors (Figure 2). The decision was made to closely monitor the patient but not to suture the stent due to severe necrosis to avoid further esophageal injury. A subsequent left gastric arteriogram was suspicious of minimal extravasation in the distal esophageal. This was empirically embolized to ensure complete hemostasis. The patient was also managed with oral pantoprazole 40 mg twice daily and sucralfate. Anticoagulation was restarted with no recurrence of bleeding. A nasogastric tube was not placed. He started eating 2 days after the EGD. We planned to remove the stent in 4 to 6 weeks. The patient was lost to follow-up. We eventually were able to contact him 3 months later. We repeated the EGD with stent removal. Complete healing of the esophageal lesion was found at that time. No complications were seen (Figure 3).
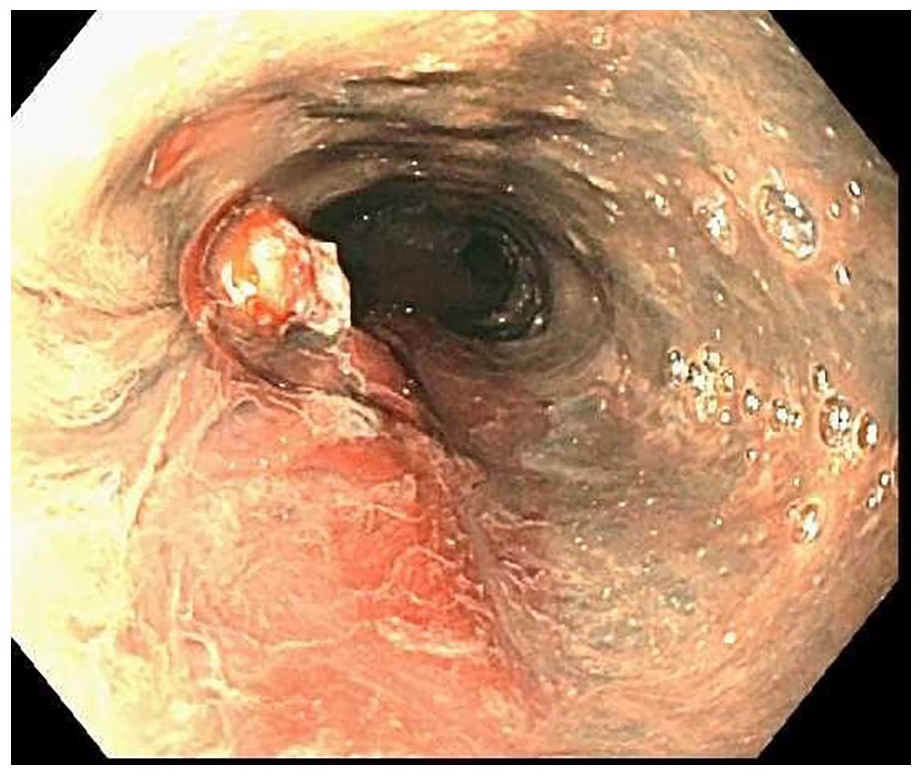
Endoscopic view of diffuse severe necrosis and black discoloration of the esophagus.

Endoscopic view of the fully covered stent placed in the esophagus.

Follow-up endoscopy showing complete healing after stent removal.
Discussion
This is a case of acute AEN managed with placement of a fully covered self-expandable stent to control bleeding. The rate of bleeding was significantly reduced after stent placement. Immediately afterward, angiogram was performed by interventional radiology. Embolization was performed to ensure complete hemostasis. AEN or necrotizing esophagitis (black esophagus) is a very rare medical condition in which the esophagus has a striking, circumferential black appearance that ends abruptly in the gastroesophageal junction. 1 In a recent review of 79 studies in which 114 patients had AEN, 2 72% of patients were men and average age was 61.2 years. The disease has an incidence of 0.01% to 0.2%, more common in men, in the sixth decade of life.3 -5 In our patient, the cause of AEN is thought to be secondary to alcohol intoxication, large IVC thrombus, and gastric acid reflux. Multiple theories are proposed to explain the pathogenesis of black esophagus, including ischemia, infections, hypothermia, gastric outlet obstruction, medications (in particular antipsychotic medications), hypercoagulable state, diabetic ketoacidosis, hypoproteinemia, cirrhosis, malignancy, and caustic injury.2,6 -9 Acute alcohol intoxication or history of chronic alcoholism could also be connected with the pathogenesis of AEN as well as gastro-esophageal reflux disease (GERD) secondary to gastric outlet obstruction, pylorus obstruction, a duodenal ulcer, or abdominal surgery. 10 Complications of AEN include bleeding, stricture formation, stenosis, perforation, and tracheoesophageal fistula formation. 2
Multiple studies and reviews agree that the initial management for AEN is supportive care, resuscitation, and proton pump inhibitors to protect the esophageal mucosa from injury from acid reflux.2,5,11 In a systematic review that included studies from 1990 to 2018, it was found that most cases of AEN were treated conservatively. Interestingly, the rate of surgical and/or endoscopic intervention (stenting or dilations to treat complications secondary to AEN) was found to be 9.7% before 2006, which increased to 30% afterward. 2 The use of a fully covered self-expandable metal stent (SEMS) has been reported for treatment of acute refractory variceal bleeding. The use of fully covered esophageal stent for management of AEN to stop bleeding was reported to avoid the risk of perforation from clipping or injection. 12 To our knowledge, this is the first case report where a fully covered SEMS was used to control bleeding in the setting of AEN.
The endoscopic intervention of SEMS represents an attractive modality for the management of a life threatening and a rare condition with a high mortality. Our case demonstrates that stenting may also help in early resumption of feeding, promote healing, and reduce the rate of complications especially perforation, stricture formation, and stenosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
For case reports or case series, our institution does not require IRB approval.
Informed Consent
We obtained a written informed consent from the patient to publish this article.
Prior Presentation
Poster presented at ACG meeting, October 2020, Virtual meeting.