
Abstract
Acute abdomen is a common emergency condition affecting young adults, and the first consideration is usually aimed to rule out acute appendicitis in this age group. Omental fat torsion has emerged as one of the rare etiologies of acute abdomen in the younger population. It warrants serious consideration as it closely mimics acute appendicitis in its clinical presentation. Herein we report a case of omental fat torsion in a 22-year-old male patient who presented with an acute right-sided lower abdominal pain which was highly suggestive of acute appendicitis. However, the diagnostic laparoscopy revealed a normally looking appendix and terminal ileum with an infarcted omental segment on the right side of the greater omentum. A laparoscopic omentectomy and an appendectomy were performed with an uneventful postoperative recovery. The pathology report confirmed omental fat infarction and a normal appendix. This case highlights omental fat infarction as a rare etiology of acute abdomen in a young male patient.
Introduction
Omental fat torsion is a rare surgical occurrence reported among younger adults presenting with acute abdomen.1 -3 Its hallmark is twisting of the omentum around its long axis, leading to intense venous congestion and then progressive arterial ischemia that eventually results in hemorrhagic fat infarction and the occurrence of omental fat necrosis. 4 The condition usually clinically presents as an acute onset of right-sided lower abdominal pain, which is, and thus simulating acute appendicitis, and less likely acute cholecystitis, right-sided diverticulitis, and acute gynecological pathologies in the female population.1-3 Preoperative diagnosis is highly challenging in this age group due to the condition’s rarity and the nonspecific nature of its clinical and laboratory findings. Hence, the vast majority of reported diagnoses are usually made intra-operatively.3,4 Most of the diagnosed cases in the reviewed literature were managed surgically with reportedly favorable long-term outcomes. The authors present a case of omental fat infarction that masqueraded clinically as acute appendicitis in a young male patient with acute right-sided lower abdominal pain. The current literature is reviewed, and we briefly discussed the epidemiology, clinicopathological features, and management of omental fat infarction in this report.
Case Presentation
A 22-year-old previously well white male patient presented to the emergency department with sudden onset of lower abdominal pain that started 2 days prior to presentation. The pain started centrally and then shifted toward the right lower abdomen and was associated with anorexia, nausea, and 2 episodes of nonbilious vomiting. His bowel habits were regular. He reported no urinary symptoms, and he has had no similar presentation with such symptoms. The review of systems was unremarkable for positive pertinent symptoms. Past medical history was insignificant.
On initial assessment, the patient looked unwell, but he was afebrile with a pulse rate of 80 beats/min and blood pressure of 110/80 mm Hg. The patient was overweight (a body mass index [BMI] of 27.8). Abdominal examination revealed focal guarding and tenderness over the right iliac fossa; the rest of the physical examination was unremarkable. Laboratory work-up revealed a total white blood count of 14 100/μL with a predominant neutrophilia (81%) and a C-reactive protein of 44 mg/dL. His urine analysis was normal. Table 1 summarizes pertinent laboratory values on admission.
Pertinent laboratory values on admission.

The patient was admitted for observation, and he was commenced on intravenous fluids and analgesia. The pain continued with increasing intensity after being observed for 8 hours. After discussion with the patient, the team decided to perform a diagnostic laparoscopy with a plan to proceed with appendectomy. Preoperative diagnostic imaging was not indicated based on the typical clinical presentation of the patient. The calculated Alvarado score was 9 out of 10, which translates to a very likely diagnosis of acute appendicitis.
Following informed consent, a diagnostic laparoscopy revealed a twisted and grossly congested segment of the greater omentum with necrotic-looking patches on exploring the omentum on the right side of the transverse colon (Figure 1). The appendix looked grossly normal (Figure 2). A further careful laparoscopic examination did not reveal any other visible pathologies in the cecum and terminal ileum (TI), small bowel, the left side of the omentum, and the pelvic cavity. A decision was made to proceed with an omentectomy of the necrotic fat segment and to perform an appendectomy to prevent the future risks of representation with acute appendicitis in this young patient. The grossly necrotic omental segment was untwisted, and then an Endoloop was applied to its base, followed by an omentectomy. A standard appendectomy was performed with no concerns.
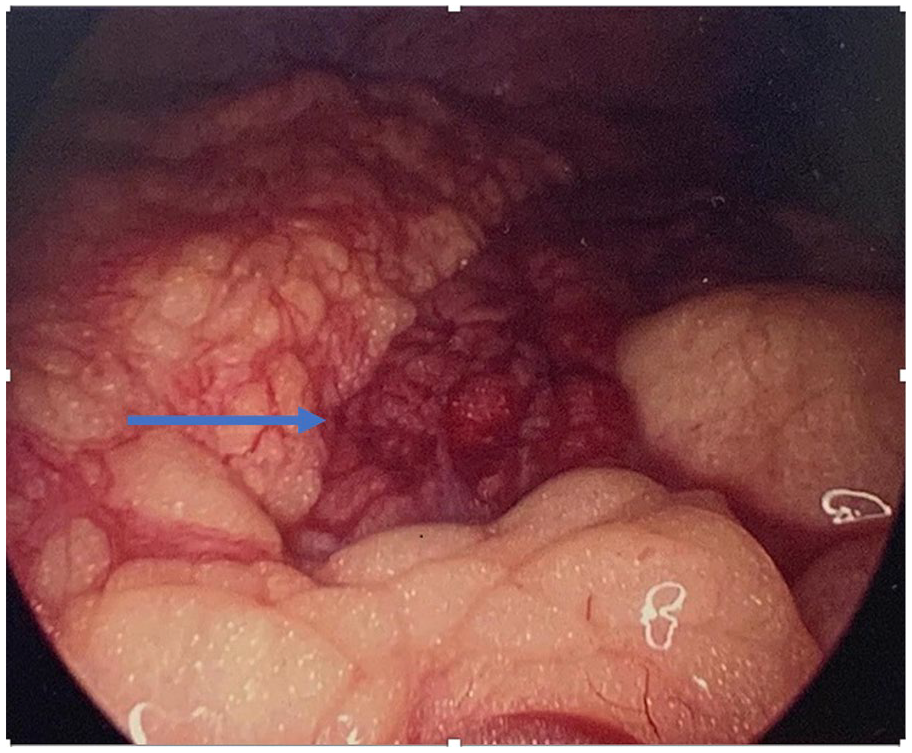
Laparoscopic visualization of a grossly congested longitudinal strip of the greater omentum on the right side of the abdomen (blue horizontal arrow), consistent with omental fat torsion with infarction.

The tip of the appendix lifted with atraumatic laparoscopic forceps, revealing a normal-looking appendix (blue horizontal arrow) and mesoappendix (blue arrowhead).
Postoperative recovery was uneventful, and the patient was discharged on the second postoperative day. The pathology report confirmed a normal appendix and demonstrated adipose tissue fragments showing ischemic and hemorrhagic changes consistent with omental fat infarction. The patient was discharged from the surgical services with no further follow-up.
Discussion
Omental fat torsion is a rare cause of acute abdominal pain in the younger adult population.1-4 The pathological types are broadly divided into a primary or secondary torsion. In primary torsion, the distal end of the omentum is free, whereas in secondary torsion, the distal end is fixed to adhesions with an underlying causative etiology.1-4
Interestingly, the most common point of omental fat torsion is around the distal right epiploic artery due to the increased length and mobility on the right side of the greater omentum, 5 and this observation would explain the predominant clinical presentation with right-sided abdominal pain resembling acute appendicitis as demonstrated in our reported patient and other similar cases.4,5
The underlying etiology of omental infarction remains poorly understood. Nevertheless, a range of precipitating factors was postulated in the reviewed literature, such as obesity, blunt abdominal trauma, and the sudden changes in body position that were thought to increase intra-abdominal pressure. 6 The reported patient was noted to be overweight (BMI of 27.8), which may have contributed to the occurrence of omental fat torsion in his case. It was theorized that the inflammatory effects of metabolically active adipose tissue might play a role in the pathogenesis of this condition. 7
The exact incidence of this condition remains largely unknown. 2 A higher incidence was reported in patients younger than 50 years as per a large retrospective series (83 cases, 52.5%) with a male to female ratio of 2:1. 2 The presumed gender-based differences could be attributed to the relatively higher fat content in the male omentum. 7 Therefore, our patient’s characteristics are in keeping with the literature.
The clinical presentation is usually localized constant pain in the right lower abdomen that is occasionally associated with low-grade fevers, vomiting, and moderate leukocytosis.4,5 About 55% of patients who were finally diagnosed with omental torsion had presented with an abdominal mass and localized peritonitis. Furthermore, those patients were observed to be less generally unwell compared with patients with appendicitis. However, most of the omental fat infarction diagnoses were made retrospectively during operative exploration in the presence of necrotic-looking omental fat and a normally looking appendix and TI. 5
A preoperative diagnosis remains challenging, as one review analyzed a total of 223 patients with omental fat infarction; the analysis revealed that an accurate preoperative diagnosis of omental fat infarction was made in 1 patient only. 8 Diagnostic imaging may help in the preoperative diagnosis in equivocal cases. 6 The typical computed tomographic (CT) appearances are hyper-attenuated fat streaks below the peritoneum in the affected segment and thickened overlying the anterior abdominal wall.5,9 Ultrasonography is generally more helpful in patients with palpable abdominal masses. The sonographic appearance is usually a hyperechoic, noncompressible mass that is reproducible with focal point tenderness. Nevertheless, diagnostic imaging was not deemed necessary in our patient, given the strong clinical suspicion of acute appendicitis. The authors believed that imaging could have been offered to aid preoperative diagnosis if the patient’s clinical presentation was rather more equivocal. Moreover, resolution of symptoms is likely to be quicker with operative management, and therefore preoperative imaging may not have changed this patient’s outcome. In addition, it avoided the risk of unnecessary exposure to radiation with abdominal CT.
In line with our approach, diagnostic laparoscopy remains the gold standard investigation in suitable patients as it is considered both a diagnostic and a therapeutic tool. 4 The usual intra-operative findings include an infarcted segment of omental fat and, less commonly, small amounts of serosanguinous fluid within the peritoneal cavity, presumably from hemorrhagic extravasation.4,5 The surgical resection of the infarcted omental segment is recommended when the diagnosis is made intra-operatively.4,7 While conservative management is advised if an imaging-confirmed preoperative diagnosis is established,4,5,7 as the condition is usually self-limiting and tends to resolve spontaneously with an extremely low incidence of reported complications. 7
It is important to note that a normal-looking appendix is usually removed—if the surgical approach is followed—to prevent potential future presentation with appendicitis and thus eliminate any possible diagnostic difficulties, in line with our team’s decision for removal.5,6 The diagnostic laparoscopy would enable an accurate visualization of the omentum in the presence of a normally looking appendix and TI, and hence is considered superior to the open approach as the latter is more challenging, especially in overweight patients to allow an adequate inspection of the peritoneal cavity. 5
Conclusion
Omental fat torsion is a rare clinical occurrence that needs to be considered as a differential diagnosis for acute right-sided abdomen in the younger male population as it closely mimics acute appendicitis in this age group. Preoperative diagnosis is extremely challenging due to its nonspecific clinical, laboratory, and radiologic findings. Hence, most diagnoses are made intra-operatively in the presence of an infarcted segment of the omental fat with a normal-looking appendix and TI. A diagnostic laparoscopy allows a thorough visualization of the peritoneal cavity in the setting of a normal appendix and TI in young patients with clinically suspected acute appendicitis. Thus, it provides a diagnostic as well as a therapeutic tool.
Learning Points
Omental fat torsion is a rare clinical entity that needs to be considered as a differential diagnosis for acute right-sided abdomen in the younger male population as it closely mimics acute appendicitis in this age group.
Preoperative diagnosis can be challenging due to the nonspecific nature of its clinical and laboratory findings, and hence most diagnoses are made intra-operatively in the presence of a normal-looking appendix and TI with an infarcted segment of the omentum.
A diagnostic laparoscopy allows a thorough visualization of the peritoneal cavity in the setting of a normal appendix and TI in young patients with clinically suspected acute appendicitis providing a diagnostic as well as a therapeutic tool.
Footnotes
Authors’ Note
This case report was presented as an abstract in the Association of Surgeons in Training Meeting, London, UK. March 2021. M Abuelgasim, A Baggaley, E Saad, 236 Omental Fat Torsion Masquerading Clinically as Acute Appendicitis in a Young Male Patient: A Rare Aetiology of Acute Abdomen and The Value of Diagnostic Laparoscopy, British Journal of Surgery, Volume 108, Issue Supplement_6, September 2021, znab259.276, ![]()
Author Contributions
The authors contributed equally to the conceptualization and designing of the report, writing the first manuscript, and critical review. All authors reviewed the last draft and agreed for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Clearance
No ethical clearance is deemed required for case report writing per our local Research Board.
Informed Consent
Informed written consent was obtained from the patient to write and publish their case as a case report with all accompanying radiological images. No identifying information has been used in this article.